
Completion requirements
MEDICALLY IMPORTANT INESTINAL HELIMINTHES, SOME CHARACTERISTICS. Quiz; Complete the table please
|
|
PARASITE |
LOCATION |
TRANSMISSION |
INFECTIVE STAGE |
MAIN DISEASE |
DIAGNOSTIC STAGE |
|
|
HELIMINTHES |
|||||
|
|
NEMATODES WITH TISSUE STAGE Soil Transmitted Heliminthes (STH) |
|||||
|
|
1. Ascaris lumbricoides |
Small intestine |
Ingestion |
Embryonated egg |
Ascriasis |
|
|
|
2. Hook worms |
Villi of small intestine |
Penetration |
Infective larva |
Hook worm disease |
|
|
|
3. Strongyloides stercoralis |
Small intestine |
Penetration |
Infective larva |
Strongyloidiasis |
|
|
|
NEMATODES WITHiot TISSUE STAGE |
|||||
|
|
4. Enterobius vermicularis |
Caecum, rectum |
Ingestion |
Embryonated egg |
Enterobiasis |
|
|
|
5. Trichuris trichiura (STH too) |
Caecum |
Ingestion |
Ebryonated egg |
Trichiriasis |
|
|
|
TAPEWORMS |
|
|
|
|
|
|
|
6. Taenia sagnata |
Small intestine |
Ingestion |
Cystcercus in beef |
Taeniasis |
|
|
|
7. Taenia solium |
Small intestine |
Ingestion |
Cyst cercus in pork |
Taeniasis & cyst cercosis |
|
|
|
8. Hymenolepsis nana |
Small intestine |
Ingestion |
Egg |
Hymenolopsis |
|
|
|
9. Diphyllobothirium latom |
Small intestine |
Ingestion |
Plerocercoid in fish |
Dyphyllobothiriasis |
|
|
|
10. Echinococcus spp E. glanulosus |
Small intestine |
Ingestion |
Embryonated eggs in faeces |
echinococcosis (hydatidosis) |
|
|
|
TREMATODES (FlUKES)
|
|
|
|
|
|
|
|
11. Fasciolopsis buski |
Duodenum & jejunum |
Ingestion |
Metacercaria on plant |
Faciolopsiasis |
|
|
|
12. Metagonimus yokogawai |
Small intestine |
Ingestion |
Metacercaria in fish |
Metagonimiasis |
|
|
|
13. Heterophyes heterophyes |
Small intestine |
Ingestion |
Metacercarie in fish |
Heterophiasis |
|
ASCARIS LUMBRICOIDES INTRODUCTION

1.Ascaris species are very large (adult females: 20 to 35 cm; adult males: 15 to 30 cm) nematodes (roundworms) that parasitize the human intestine.
2.A. lumbricoides is the primary species involved in human infections globally, but Ascaris derived from pigs (often referred to as A. suum) may also infect humans.
3.These two parasites are very closely related, and hybrids have been identified; thus, their status as distinct, reproductively isolated species is a contentious topic.
ASCARIS LUMBRICOIDES DISTRIBUTION
1.Ascaris lumbricoides infections happen all over the world.
2.Most cases occur in tropical and subtropical areas of Asia, sub-Saharan Africa, and the Americas
ASCARIS LUMBRICOIDES TRANSMISSION & LIFE CYCLE
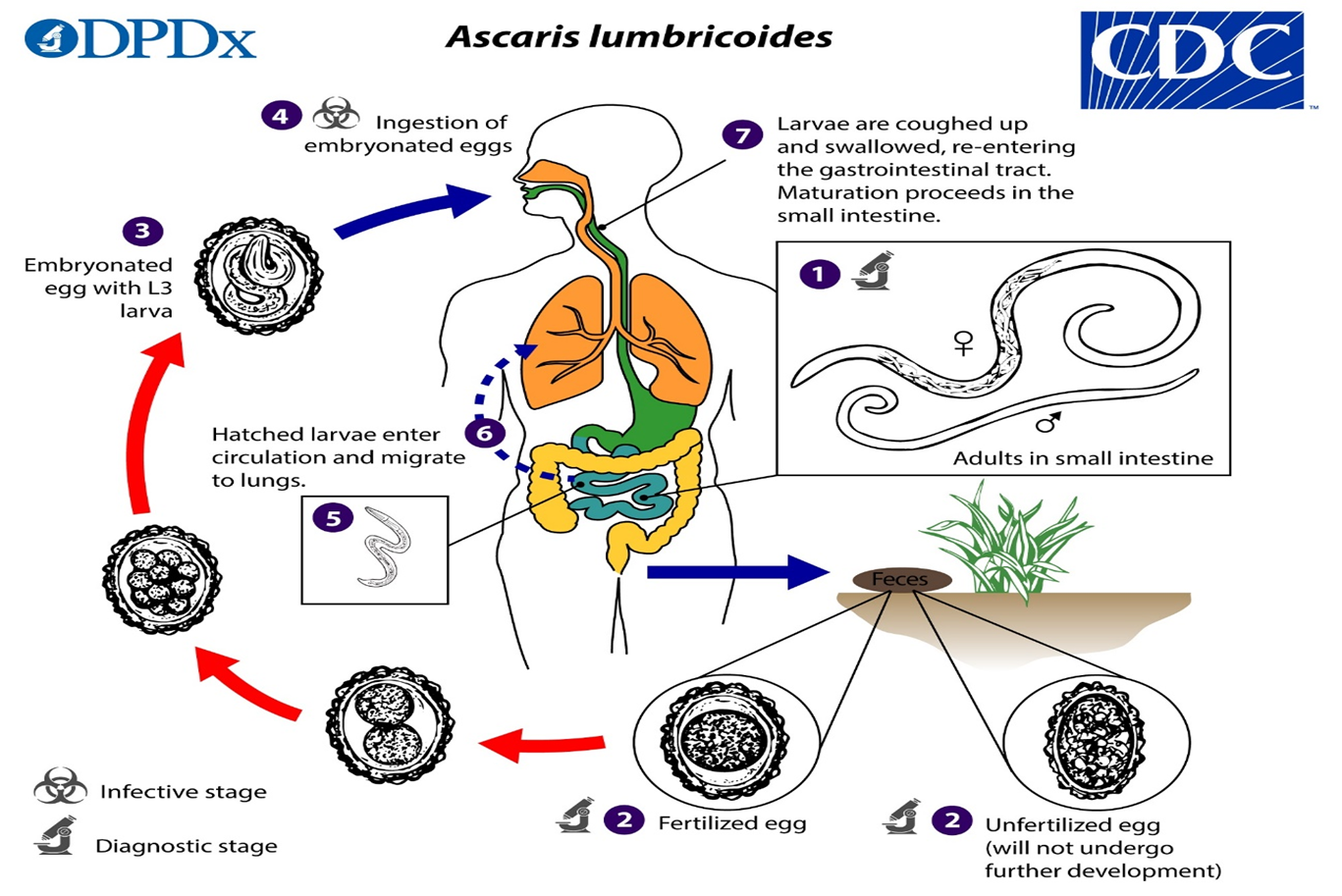
1.Adult worms live in the lumen of the small intestine. A female may produce approximately 200,000 eggs per day, which are passed with the feces.
2.Unfertilized eggs may be ingested but are not infective.
3.Larvae develop to infectivity within fertile eggs after 18 days to several weeks, depending on the environmental conditions (optimum: moist, warm, shaded soil).
4. After infective eggs are swallowed,
5. Larvae hatch
6.Invade the intestinal mucosa, and are carried via the portal, then systemic circulation to the lungs. The larvae mature further in the lungs (10 to 14 days), penetrate the alveolar walls, ascend the
bronchial tree to the throat, and are swallowed.
7.Upon reaching the small intestine, they develop into adult worms. Between 2 and 3 months are required from ingestion of the infective eggs to oviposition by the adult female. Adult worms can live 1 to 2 years.
ASCARIS LUMBRICOIDES PATHOGENESIS AND CLINICAL PRESENTATION
1.People infected with Ascaris often show no symptoms, regardless of the species of worm.
2.If symptoms do occur they can be light and include abdominal discomfort.
3.Heavy infections can cause intestinal blockage and impair growth in children.
4.Other symptoms such as cough are due to migration of the worms through the body.
ASCARIS LUMBRICOIDES LAB DIAGNOSIS
1.The standard method for diagnosing ascariasis is by identifying Ascaris eggs in a stool sample using a microscope.
2.Because eggs may be difficult to find in light infections, a concentration procedure is recommended.
ASCARIS LUMBRICOIDES TREATMENT
1.Albendazole and mebendazole, are the drugs of choice for treatment of Ascaris infections, regardless of the species of worm.
2.Infections are generally treated for 1–3 days.
3.The drugs are effective and appear to have few side effects.
ASCARIS LUMBRICOIDES PREVENTION AND CONTROL MEASURES
1.Health education on transmission routes and contamination of environment
2.Effective sewage disposal systems
3.Personal hygiene to prevent food, water, and hands becoming contaminated with human or pig feces, including where human fecal matter (“night soil”), wastewater, or pig manure is used to fertilize crops
4.Wash, peel, or cook all raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with manure.
5.Early laboratory diagnosis and treatment of the infected person
HOOK WORM INTRODUCTION
1.Intestinal hookworm disease in humans is caused by Ancylostoma duodenale, A. ceylanicum, and Necator americanus.
2.Classically, A. duodenale and N. americanus were considered the two primary intestinal hookworm species worldwide, but newer studies show that a parasite infecting animals, A. ceylanicum, is also an important emerging parasite infecting humans in some regions.
3.Occasionally larvae of A. caninum, normally a parasite of canids, may partially develop in the human intestine and cause eosinophilic enteritis, but this species does not appear to reach reproductive maturity in humans.
HOOK WORM DISTRIBUTION
Ancylostoma duodenale and Necator americanus, are worldwide in areas with warm, moist climates and are widely overlapping.
HOOK WORM TRANSMISSION AND LIFE CYCLE
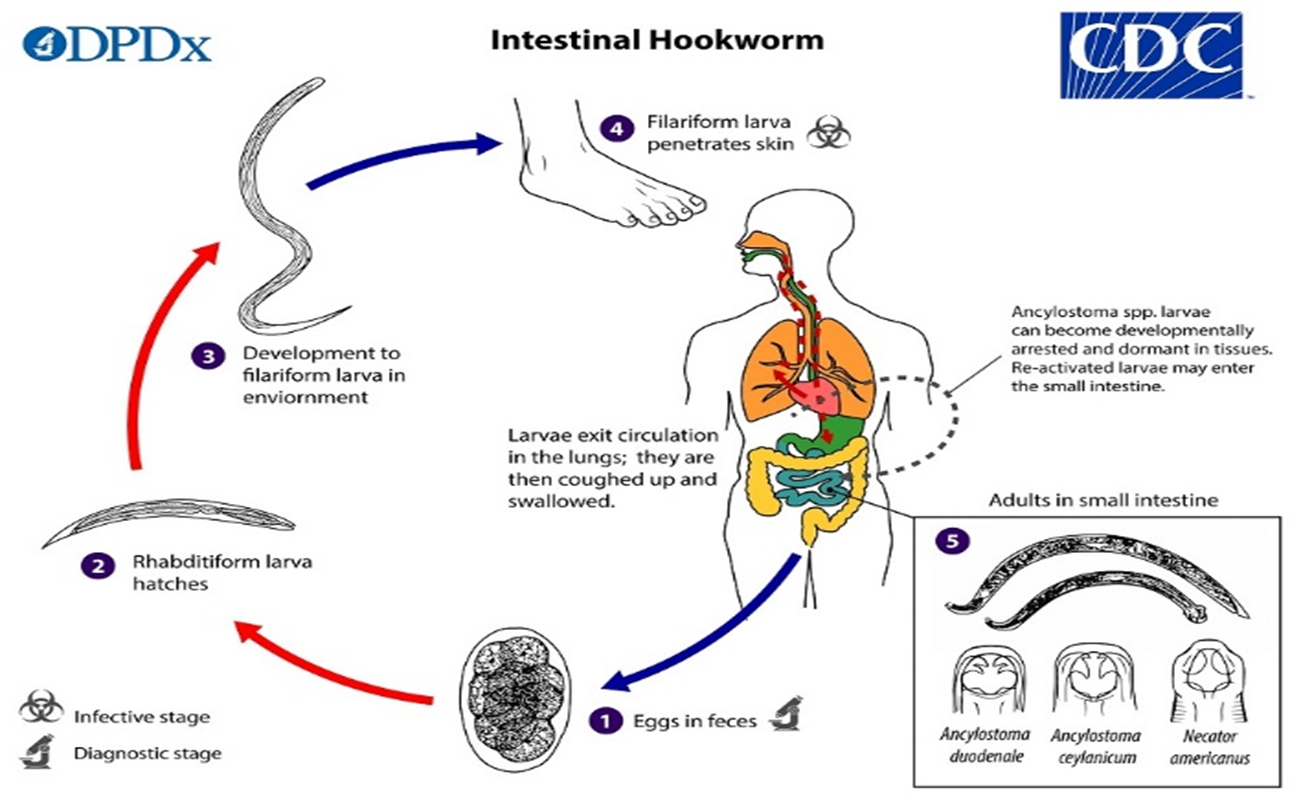
1.Eggs are passed in the stool, and under favorable conditions (moisture, warmth, shade), larvae hatch in 1 to 2 days and become free-living in contaminated soil.
2.These released rhabditiform larvae grow in the feces and/or the soil, and after 5 to 10 days (and two molts) they become filariform (third-stage) larvae that are infective.
3.These infective larvae can survive 3 to 4 weeks in favorable environmental conditions. On contact with the human host, typically bare feet, the larvae penetrate the skin and are carried through the blood vessels to the heart and then to the lungs.
4.They penetrate into the pulmonary alveoli, ascend the bronchial tree to the pharynx, and are swallowed.
5.The larvae reach the jejunum of the small intestine, where they reside and mature into adults. Adult worms live in the lumen of the small intestine, typically the distal jejunum, where they attach to the intestinal wall with resultant blood loss by the host.
6.Most adult worms are eliminated in 1 to 2 years, but the longevity may reach several years.
HOOK WORM PATHOGENESIS AND CLINICAL PRESENTATION
1.The most serious effects of hookworm infection are the development of anemia and protein deficiency caused by blood loss at the site of the intestinal attachment of the adult worms.
2.When children are continuously infected by many worms, the loss of iron and protein can retard growth and mental development.
HOOK WORM LAB DIAGNOSIS
1.The standard method for diagnosing the presence of hookworm is by identifying hookworm eggs in a stool sample using a microscope.
2.Because eggs may be difficult to find in light infections, a concentration procedure is recommended.
HOOK WORM TREATMENT
1.Albendazole and mebendazole, are the drugs of choice for treatment of hookworm infections.
2.Infections are generally treated for 1-3 days.
3.The recommended medications are effective and appear to have few side effects.
4.Iron supplements may also be prescribed if the infected person has anemia.
HOOK WORM PREVENTION AND CONTROL
1.Health education on transmission routes and contamination of environment
2.Effective sewage disposal systems
3.Not to walk barefoot in areas where hookworm is common and where there may be human fecal contamination of the soil.
4.Also, avoid other skin contact with such soil and avoid ingesting it.
5.Early laboratory diagnosis and treatment of the infected person
STRONGYLOIDES STERCORALIS INTRODUCTION
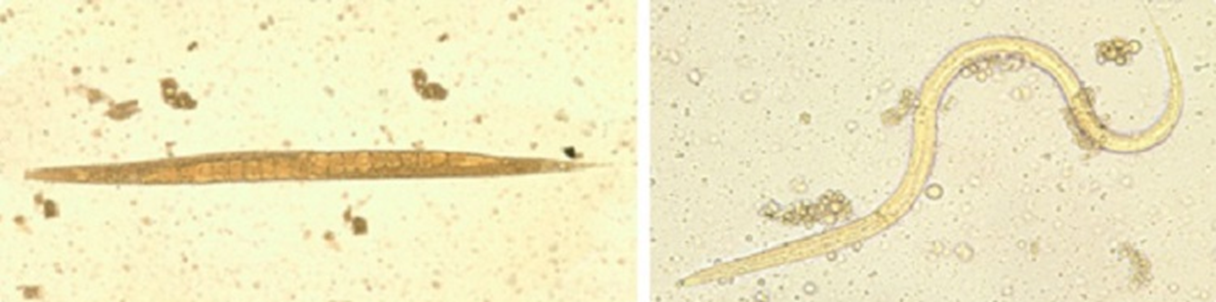
Right: Filariform (L3) larva of S. stercoralis in an unstained wet mount. (Credit: DPDx)
Left: Free living spp.
1.The rhabditid nematode (roundworm) Strongyloides stercoralis is the major causative agent of strongyloidiasis in humans.
2.Thread worm is sometimes, in some countries, also used to refer to Strongyloides stercoralis like with Enterobius vermicularis.
3.Rarer human-infecting species of Strongyloides are the zoonotic S. fuelleborni (fülleborni) subsp. fuelleborni and
4.S. fuelleborni subsp. kellyi, the only currently known host is humans.
STRONGYLOIDES STERCORALIS DISTRIBUTION
1.Strongyloides stercoralis is broadly distributed in tropical and subtropical areas across the globe.
2.The vast majority of human infections are reported from sub-Saharan Africa.
3.Sporadic cases have been reported from Southeast Asia. S. fuelleborni subsp. kellyi is found in Papua New Guinea, and has not been reported elsewhere thus far.
STRONGYLOIDES STERCORALIS TRANSMISSION AND LIFE CYCLE
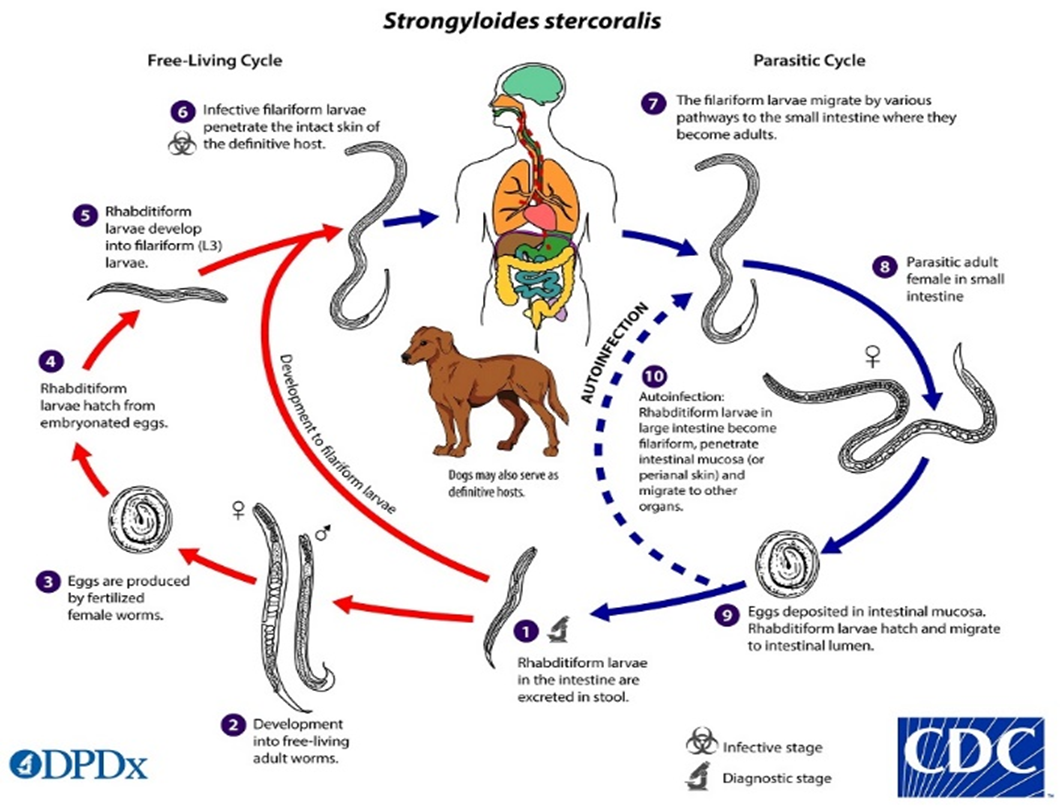
The Strongyloides stercoralis life cycle is complex, alternating between free-living and parasitic cycles and involving autoinfection.
In the free-living cycle:
1. Rhabditiform larvae are passed in the stool of an infected definitive host, develop into either infective filariform larvae (direct development), or free-living adult males and females
2.that mate and produce eggs
3.from which rhabditiform larvae hatch
4.and eventually become infective filariform (L3) slarvae
5.The filariform larvae penetrate the human host skin to initiate the parasitic cycle (see below)
6.This second generation of filariform larvae cannot mature into free-living adults and must find a new host to continue the life cycle.
In the parasitic cycle:
6.Filariform larvae in contaminated soil penetrate human skin when skin contacts soil ,
7.And migrate to the small intestine
8.It has been thought that the L3 larvae migrate via the bloodstream and lymphatics to the lungs, where they are eventually coughed up and swallowed. However, L3 larvae appear capable of migrating to the intestine via alternate routes (e.g. through abdominal viscera or connective tissue). In the small intestine, the larvae molt twice and become adult female worms,
In the autoinfection cycle:
9.The females live embedded in the submucosa of the small intestine and produce eggs via parthenogenesis (parasitic males do not exist),
10.Which yield rhabditiform larvae. The rhabditiform larvae can either be passed in the stool,
11.(see “Free-living cycle” above), or can cause autoinfection.
12.Once the filariform larvae reinfect the host, they are carried to the lungs, pharynx and small intestine as described above, or disseminate throughout the body.
13.Strongyloides fuelleborni follows the same life cycle as S. stercoralis,w the important distinction that eggs not larvae are passed in the stool
STRONGYLOIDES STERCORALIS PATHOGENISIS AND CLINICAL PRESENTATION
Most people infected with Strongyloides do not know they are infected. If they do feel sick the most common complaints are the following:
1.Abdominal
2.Stomachache, bloating, and heartburn
3.Intermittent episodes of diarrhea and constipation
4.Nausea and loss of appetite
5.Dry cough
6.Throat irritation
7.An itchy, red rash that occurs where the worm entered the skin
8. Recurrent raised red rash typically along the thighs and buttocks9.Rarely, severe life-threatening forms of the disease called hyperinfection syndrome and disseminated strongyloidiasis can occur.
These forms of the disease are more common in people who are on corticosteroids (for example, prednisone) or other immunosuppressive therapies or who are infected with HTLV-1. In this situation, people become critically ill, and should be taken to the hospital immediately.
STRONGYLOIDES STERCORALIS LAB DIAGNOSIS
1.The standard method for Strongyloides infection diagnosis stool examined under the microscope, but it might not find the worms in all infected people.
2.This may require provision of multiple stool samples.
3.Concentration procedures may be recommended.
STRONGYLOIDES STERCORALIS TREAMENT
1.Ivermectin, Relative contraindications include the following: Confirmed or suspected concomitant Loa loa infection, Persons weighing less than 15kg, Pregnant or lactating women
2.Albendazole
STRONGYLOIDES STERCORALIS PREVENTION AND CONTROL
1.Health education on transmission routes and contamination of environment
2.Effective sewage disposal systems
3.Not to walk barefoot in areas where strongyloides ae common and where there may be human fecal contamination of the soil.
4.Also, avoid other skin contact with such soil and avoid ingesting it.
5.Early laboratory diagnosis and treatment of the infected person
ENTEROBIUS VERMICULARIS INTRODUCTION
1.The nematode (roundworm) Enterobius vermicularis is widely known as the human pinworm due to the female’s long, pointed tail.
2.In some areas the common names “seatworm” and “threadworm” are used (the latter of which is sometimes also used to refer to strongyloides stercoralis.
3.Another putative pinworm species, Enterobius gregorii, has been described and reported from humans in Europe, Africa, and Asia. However, further morphologic and molecular evidence suggests E. gregorii likely represents an immature form of E. vermicularis.
4.The rat pinworm, Syphacia obvelata, has also very rarely been reported infecting humans.
ENTEROBIUS VERMICULARIS DISTRIBUTION
E. vermicularis occurs worldwide, with infections occurring most frequently in school- or preschool-children and in crowded conditions
ENTEROBIUS VERMICULARIS TRANSMISSION AND LIFE CYCLE
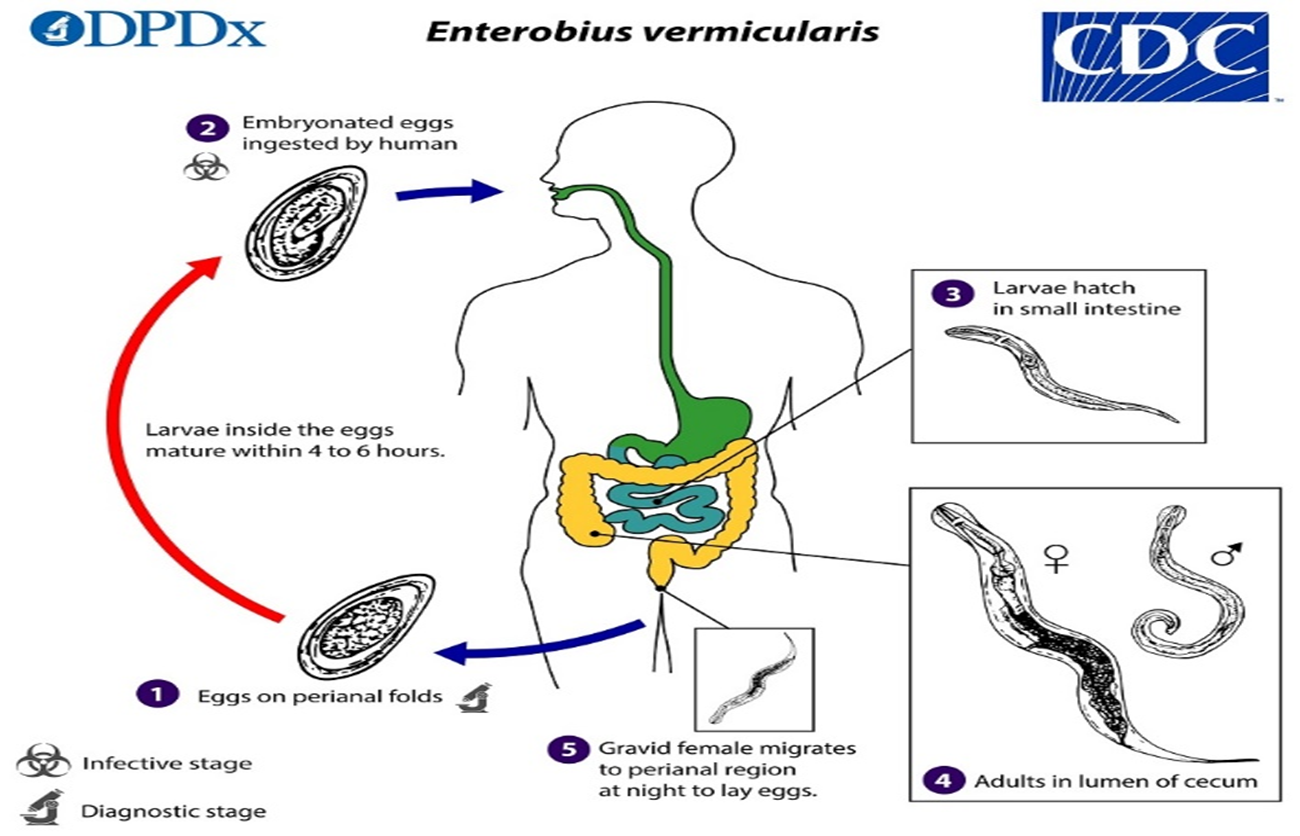
Gravid adult female Enterobius vermicularis deposit eggs on perianal folds.
1.Infection occurs via self-inoculation (transferring eggs to the mouth with hands that have scratched the perianal area) or through exposure to eggs in the environment (e.g. contaminated surfaces, clothes, bed linens, etc.)
2.Following ingestion of infective eggs, the larvae hatch in the small intestine
3.and the adults establish themselves in the colon, usually in the cecum.
4.The time interval from ingestion of infective eggs to oviposition by the adult females is about one month. At full maturity adult females measure 8 to 13 mm, and adult males 2 to 5 mm; the adult life span is about two months. Gravid females migrate nocturnally outside the anus and oviposit while crawling on the skin of the perianal area.
5.The larvae contained inside the eggs develop (the eggs become infective) in 4 to 6 hours under optimal conditions.
Rarely, eggs may become airborne and be inhaled and swallowed. Retroinfection, or the migration of newly hatched larvae from the anal skin back into the rectum, may occur but the frequency with which this happens is unknown.ENTEROBIUS VERMICULARIS PATHOGENESIS AND CLINICAL PRESENTATION
1.The most common clinical manifestation of a pinworm infection is an itchy anal region.
2.When the infection is heavy, there can be a secondary bacterial infection due to the irritation and scratching of the anal area.
3.Often the patient will complain of teeth grinding, and insomnia due to disturbed sleep, or even abdominal pain or appendicitis.
4.Infection of the female genital tract has been well reported.
ENTEROBIUS VERMICULARIS LAB DIAGNOSIS
1.Is to look for the worms in the perianal reqion 2 to 3 hours after the infected person is asleep.
2.Is to touch the perianal skin with transparent tape to collect possible pinworm eggs around the anus first thing in the morning. If a person is infected, the eggs on the tape will be visible under a microscope. The tape method should be conducted on 3 consecutive mornings immediately after the infected person wakes up.
3.Is analyzing samples from under fingernails under a microscope, since anal itching is a common symptom of pinworm.
Examining stool samples is not recommended. Since pinworm eggs and worms are often sparse in stool.
ENTEROBIUS VERMICULARIS TREATMENT
1.The medications used for the treatment of pinworm are either mebendazole, pyrantel pamoate, or albendazole.
2.Any of these drugs are given in one dose initially, and then another single dose of the same drug two weeks later. Pyrantel pamoate is available without prescription.
3.The medication does not reliably kill pinworm eggs. Therefore, the second dose is to prevent re-infection by adult worms that hatch from any eggs not killed by the first treatment.
4.Health practitioners and parents should weigh the health risks and benefits of these drugs for patients under 2 years of age.
ENTEROBIUS VERMICULARIS PREVENTION AND CONTROL
1.Health education on transmission routes and contamination of environment
2.Frequent changing of underclothes, bed linens and changing diapers, first thing in the morning is a great way to prevent possible transmission of eggs in the environment and risk of reinfection.
3.These items should not be shaken and carefully placed into a washer and laundered in hot water followed by a hot dryer to kill any eggs that may be there.
4.Showering every morning is a better method than taking a bath, in case of bathing infected people should not co-bathe with others during their time of infection.
5.Good hygiene practices such as washing your hands with soap and warm water after using the toilet, and before handling food is the most successful way to prevent pinworm infection.
6.Cut fingernails regularly, and avoid biting the nails and scratching around the anus.
7.Early laboratory diagnosis and treatment of the infected person
TRICHURIS TRICHIURA INTRODUCTION

The nematode (roundworm) Trichuris trichiura, also called the human whipworm.
TRICHURIS TRICHIURA DISTRIBUTION
1.Worldwide, infection occurs more frequently in areas with tropical weather, where access to personal hygiene and proper sanitation practices are not available, and among children.
2.Whipworm is a soil-transmitted helminth (STH) and is the third most common roundworm of humans.
TRICHURIS TRICHIURA TRANSMISSION AND LIFE CYCLE
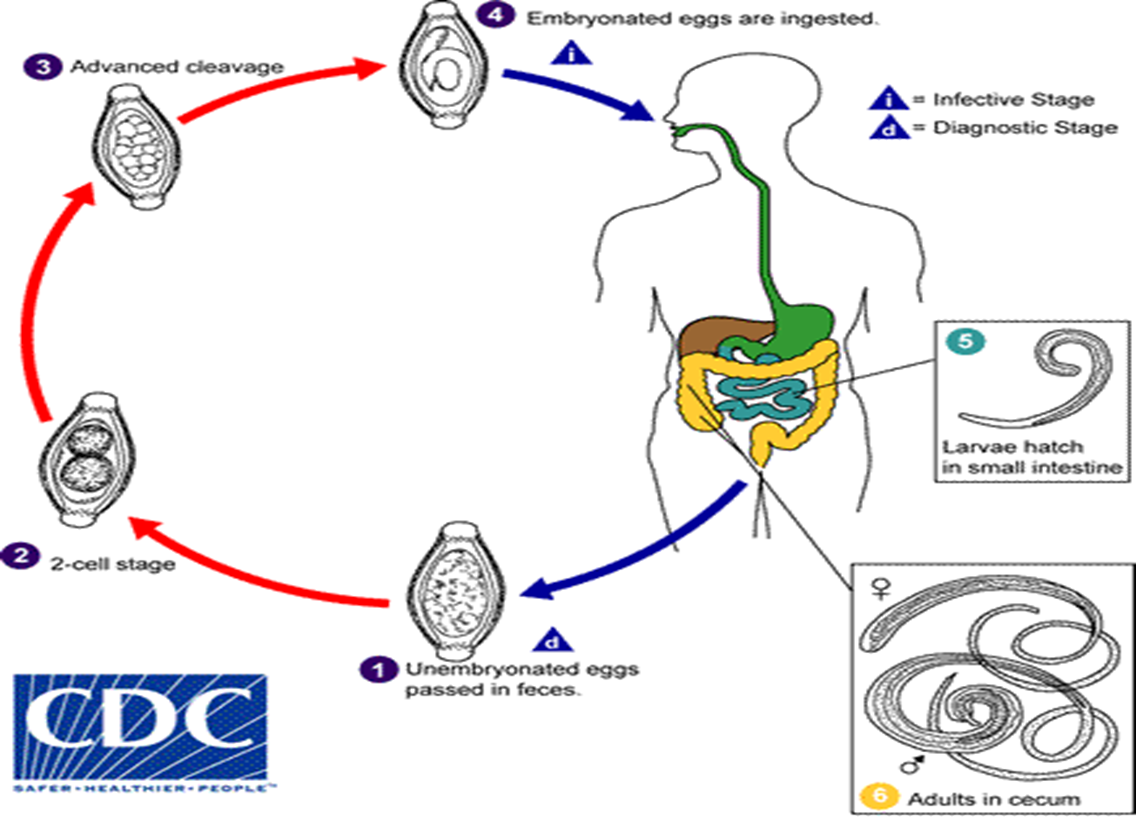
1. The unembryonated eggs are passed with the stool
2. In the soil, the eggs develop into a 2-cell stage
3. an advanced cleavage stage and then they embryonate the eggs become infective in 15 to 30 days.
4. After ingestion (soil-contaminated hands or food),
5. the eggs hatch in the small intestine, and release larvae
6. that mature and establish themselves as adults in the colon
7. The adult worms (approximately 4 cm in length) live in the cecum and ascending colon. The adult worms are fixed in that location, with the anterior portions threaded into the mucosa.
8. The females begin to oviposit 60 to 70 days after infection. Female worms in the cecum shed between 3,000 and 20,000 eggs per day.
9. The life span of the adults is about 1 year.
TRICHURIS TRICHIURA PATHOGENESIS AND CLINICAL PRESENTATION
1. People infected with whipworm can suffer light or heavy infections.
2. People with light infections usually have no symptoms.
3. People with heavy symptoms can experience frequent, painful passage of stool that contains a mixture of mucus, water, and blood.
4. Rectal prolapse can also occur.
5. Heavy infection in children can lead to severe anemia, growth retardation, and impaired cognitive development.
TRICHURIS TRICHIURA LAB DIAGNOSIS
1. The standard method for diagnosing the presence of whipworm is by microscopically identifying whipworm eggs in a stool sample.
2. Because eggs may be difficult to find in light infections, a concentration procedure is recommended.
TRICHURIS TRICHIURA TREATMENT
1. Albendazole and mebendazole, are the drugs of choice for treatment.
2. Infections are generally treated for 3 days.
3. Iron supplements may also be prescribed if the infected person suffers from anemia.
TRICHURIS TRICHIURA PREVENTION AND CONTROL
1. Health education on transmission routes and contamination of environment
2. Effective sewage disposal systems
3. Personal hygiene to prevent food, water, and hands becoming contaminated with human feces, including where human fecal matter (“night soil”), wastewater, used to fertilize crops
4. Wash, peel, or cook all raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with night soil.
5. Early laboratory diagnosis and treatment of the infected person
TWENIA SAGNATA AND TAENIA SOLIUM INTRODUCTION
1. The cestodes (tapeworms) Taenia saginata (beef tapeworm) and T. solium and T. asiatic (pork tapeworm).
2. Taeniasis is the infection of humans with the adult tapeworm of Taenia saginata or Taenia solium.
3. Humans are the only definitive hosts for T. saginata and T. solium.
4. Taenia solium eggs can also cause cysticercosis.
5. Length of adult worms is usually 5 m or less for T. saginata (however it may reach up to 25 m) and 2 to 7 m for T. solium.
TWENIA SAGNATA AND TAENIA SOLIUM DISTRIBUTION
1. The tapeworms that cause taeniasis (Taenia saginata, T. solium, and T. asiatica) are found worldwide.
2. Both the tapeworm infection, also known as taeniasis, and cysticercosis occur globally.
3. The highest rates of infection are found in areas of Latin America, Asia, Eastern Europe, sub-Saharan Africa, India, that have poor sanitation and free-ranging pigs that have access to human feces.
TWENIA SAGNATA AND TAENIA SOLIUM TRANSMISSION AND LIFE CYCLE
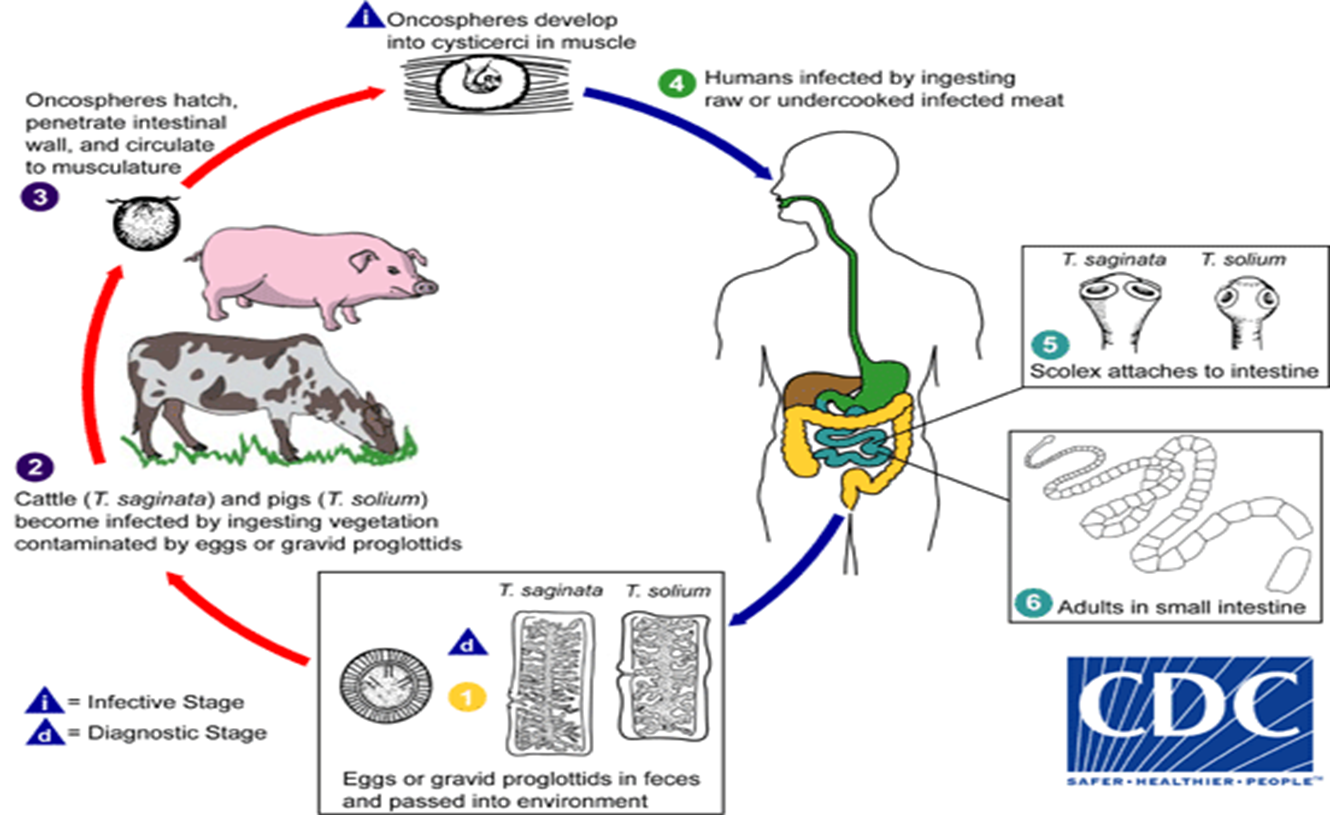
1. Eggs or gravid proglottids are passed with feces; the eggs can survive for days to months in the environment.
2. Cattle (T. saginata) and pigs (T. solium) become infected by ingesting vegetation contaminated with eggs or gravid proglottids.
3. In the animal’s intestine, the oncospheres hatch, invade the intestinal wall, and migrate to the striated muscles, where they develop into cysticerci. A cysticercus can survive for several years in the animal.
4. Humans become infected by ingesting raw or undercooked infected meat. In the human intestine, the cysticercus develops over 2 months into an adult tapeworm, which can survive for years.
5. The adult tapeworms attach to the small intestine by their scolex and reside in the small intestine.
6. The adults produce proglottids which mature, become gravid, detach from the tapeworm, and migrate to the anus or are passed in the stool (approximately 6 per day). T. saginata adults usually have 1,000 to 2,000 proglottids, while T. solium adults have an average of 1,000 proglottids. The eggs contained in the gravid proglottids are released after the proglottids are passed with the feces. T. saginata may produce up to 100,000 and T. solium may produce 50,000 eggs per proglottid respectively.
TWENIA SAGNATA AND TAENIA SOLIUM PATHOGENESIS AND CLICAL PRESENTATION
1. Most people with tapeworm infections have no symptoms or mild symptoms.
2. Patients with T. saginata taeniasis often experience more symptoms than those with T. solium because the T. saginata tapeworm is larger in size (up to 10 meters (m)) than T. solium (usually 3 m).
3. Tapeworms can cause digestive problems including abdominal pain, loss of appetite, weight loss, and upset stomach.
4. The most visible symptom of taeniasis is the active passing of proglottids (tapeworm segments) through the anus and in the feces.
5. In rare cases, tapeworm segments become lodged in the appendix, or the bile and pancreatic ducts.
6. cystcercosis a parasitic tissue infection caused by larval cysts of the tapeworm Taenia solium.
i. These larval cysts infect brain, muscle, or other tissue, and are a major cause of adult onset seizures in most low-income countries.
ii. A person gets cysticercosis by swallowing eggs found in the feces of a person who has an intestinal tapeworm. People do not get cysticercosis by eating undercooked pork.
iii. People living in the same household with someone who has a tapeworm have a much higher risk of getting cysticercosis than people who don’t.
TWENIA SAGNATA AND TAENIA SOLIUM LAB DIAGNOSIS
1. The standard method for diagnosing the presence of taenisis is by microscopically identifying taenia spp eggs in a stool sample.
2. Because eggs may be difficult to find in light infections, a concentration procedure is recommended.
3. The diagnosis of neurocysticercosis usually requires MRI or CT brain scans.
4. Blood tests may be useful to help diagnose an infection, but they may not always be positive in light infections.
TWENIA SAGNATA AND TAENIA SOLIUM TREATMENT
1. Praziquantel is the medication most often used to treat active taeniasis,
2. Altanatives: Niclosamide and Albendazole
3. Some people with cysticercosis do not need to be treated. Sometimes surgery may be needed.
TWENIA SAGNATA AND TAENIA SOLIUM TREATMENT
1. Health education on transmission routes and contamination of environment
2. Effective sewage disposal systems
3. Personal hygiene to prevent food, water, and hands becoming contaminated with human feces, including where human fecal matter (“night soil”), wastewater, used to fertilize crops
4. Cook all meat properly and cook, wash, peel, raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with night soil and manure.
5. Early laboratory diagnosis and treatment of the infected person
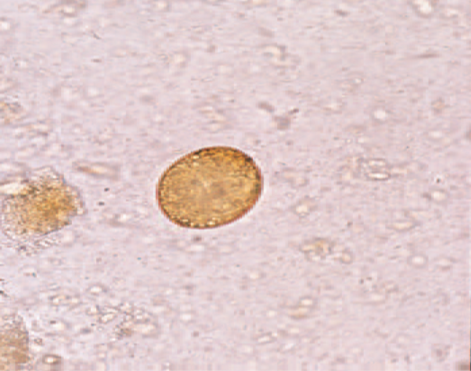
HYMENOLEPIS NANA INTRODUCTION

Images: Left: H. nana egg in an unstained wet mount.
(Credit: DPDx, Georgia Department of Public Health, Dr.David Bruckner)
- Hymenolepis nana (the dwarf tapeworm is a cestode (tapeworm), adults measuring 15 to 40 mm in length).
HYMENOLEPIS NANA TRANSMISSION AND LIFE CYCLE
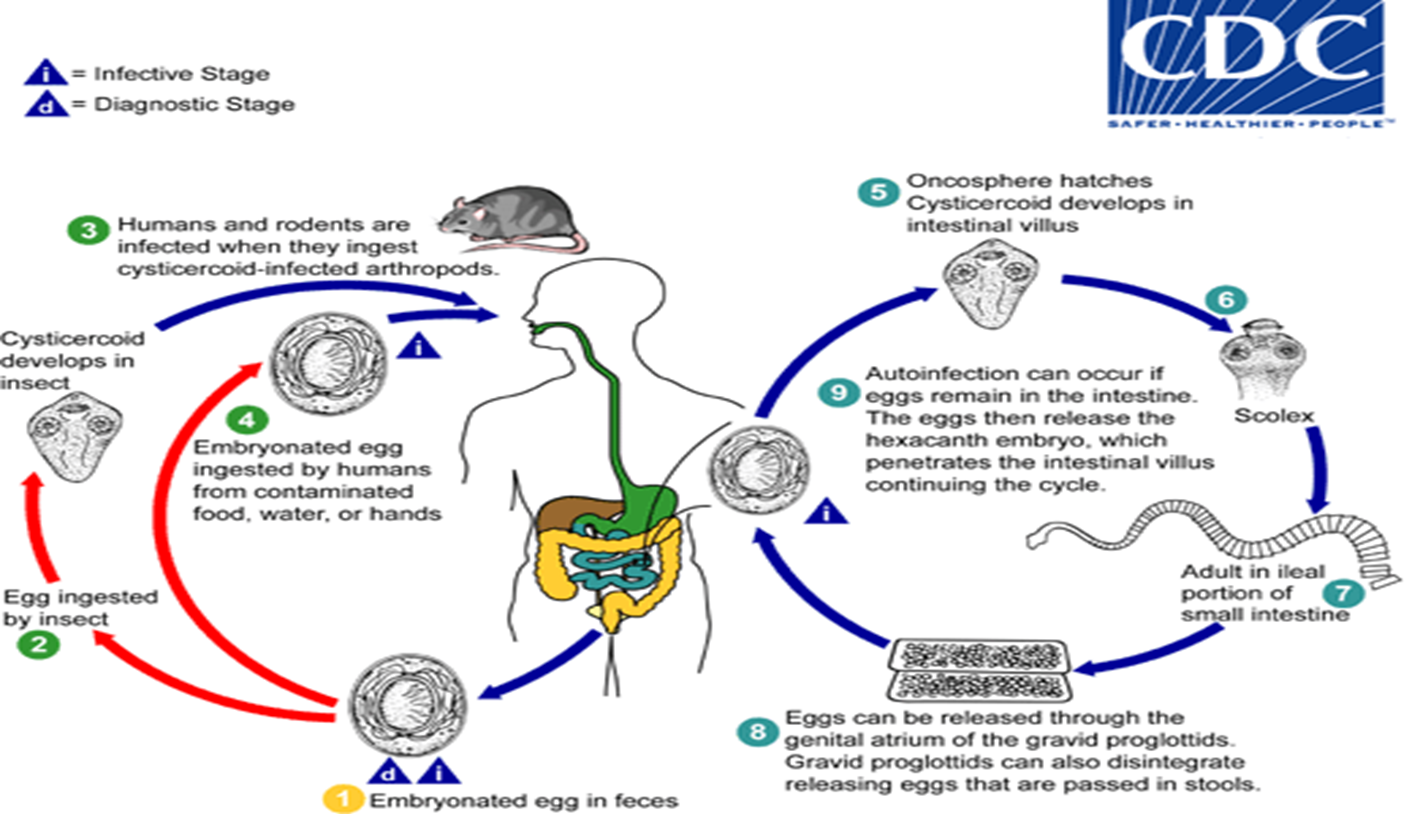
1. Eggs of Hymenolepis nana are immediately infective when passed with the stool and cannot survive more than 10 days in the external environment.
2. When eggs are ingested by an arthropod intermediate host (various species of beetles and fleas may serve as intermediate hosts), they develop into cysticercoids,
3. which can infect humans or rodents upon ingestion and develop into adults in the small intestine. A morphologically identical variant, H. nana var. fraterna, infects rodents and uses arthropods as intermediate hosts.
9. An alternate mode of infection consists of internal autoinfection, where the eggs release their hexacanth embryo, which penetrates the villus continuing the infective cycle without passage through the external environment.
10. The life span of adult worms is 4 to 6 weeks, but internal autoinfection allows the infection to persist for years.
HYMENOLEPIS NANA PATHOGENESIS AND CLINICAL PRESENTATION
1. Most people who are infected do not have any symptoms.
2. Those who have symptoms may experience nausea, weakness, loss of appetite, diarrhea, and abdominal pain.
3. Young children, especially those with a heavy infection, may develop a headache, itchy bottom, or have difficulty sleeping.
HYMENOLEPIS NANA LAB DIAGNOSIS
1. The standard method for diagnosing the presence of Hymenolopis nana is by microscopically identifying its eggs in a stool sample.
2. Because eggs may be difficult to find in light infections, a concentration procedure is recommended.
HYMENOLEPIS NANA TREATMENT
Praziquantel is the medication most often used to treat Hymenolopsis nana infection.
HYMENOLEPIS NANA PREVENTION AND CONTROL
1. Health education on transmission routes and contamination of environment
2. Effective sewage disposal systems
3. Personal hygiene to prevent food, water, and hands becoming contaminated with human feces, including where human fecal matter (“night soil”), wastewater, used to fertilize crops
4. Cook, wash, peel, raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with night soil.
5. Early laboratory diagnosis and treatment of the infected person
DIPHYLLOBOTHIRIUM LATUM INTRODUCTION
1. Diphyllobothrium latum and related species (the fish or broad tapeworm), are the largest tapeworms that can infect people.
2. These pseudophyllidean cestodes have a scolex bearing bothria (grooves), instead of suckers.
3. Definitive hosts include fish-eating carnivores, but humans are the important hosts.
4. D. latum adults can reach more than 10 m in length, with more than 3,000 proglottids.
5. Recent research incorporating morphologic and molecular data has led to the re-classification and re-naming of most of the human-infecting diphyllobothriids. Dibothriocephalus latus (=Diphyllobothrium latum),
6. However, it is possible that many historical cases were falsely attributed to this species. Dibothriocephalus nihonkaiense (=Diphyllobothrium nihonkaiense), Dibothriocephalus dendriticus (=Diphyllobothrium dendriticum), Diphyllobothrium stemmacephalum (=Diphyllobothrium stemmacephalum; =Diphyllobothrium yonagoense), Diphyllobothrium balaenopterae (=Diplogonoporus grandis; =Diplogonoporus balaenoptera), and Adenocephalus pacificus (=Diphyllobothrium pacificum) are also known to infect humans.
DIPHYLLOBOTHIRIUM LATUM DISTRIBUTION
1. D. latum is widely distributed in the lake areas of Europe, North America and the Far East. It is also found in parts of Asia and South America.
2. But cases have also been reported in Uganda and Chile
DIPHYLLOBOTHIRIUM LATUM TRANSMISSION AND LIFE CYCLE
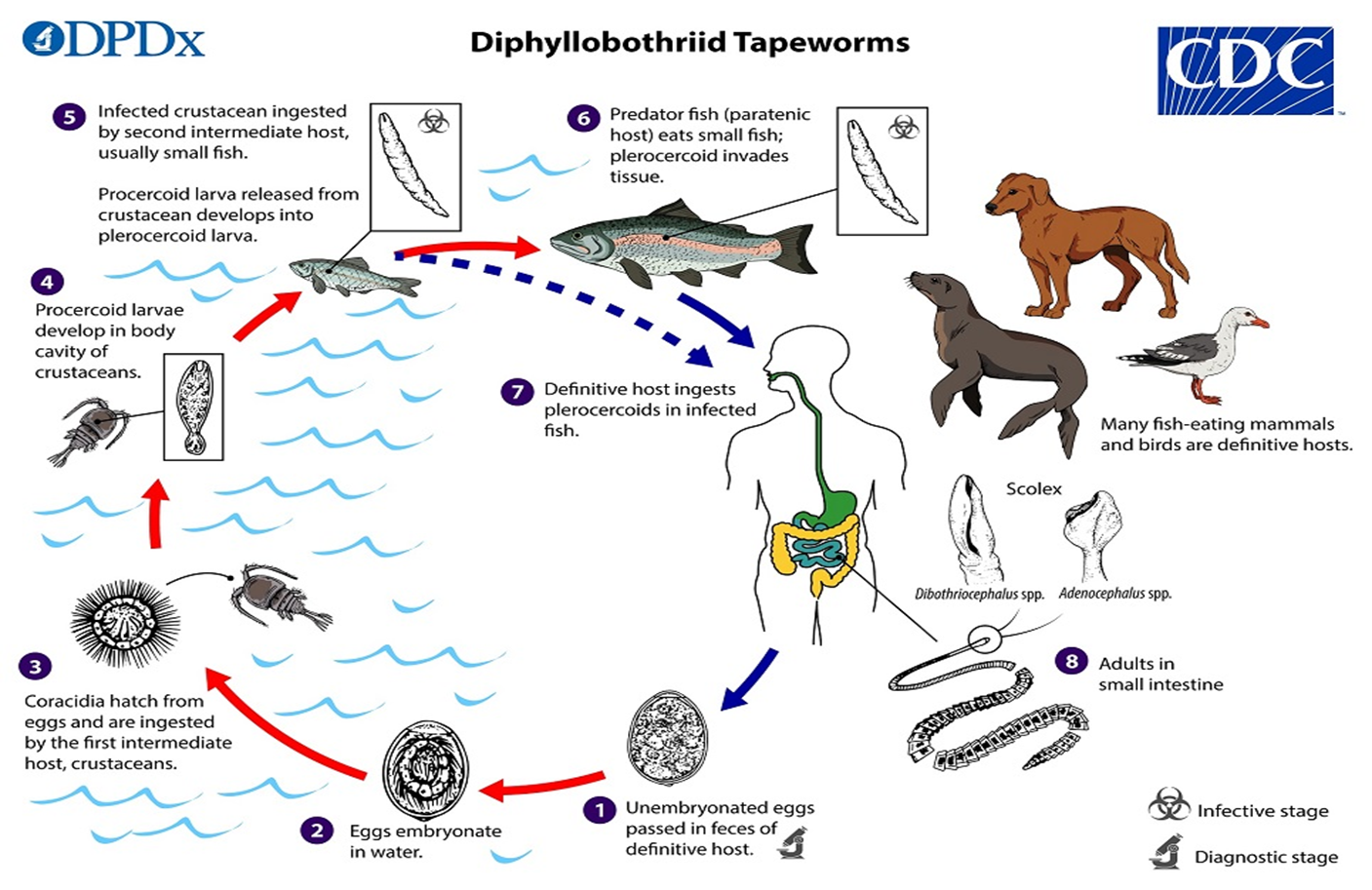
1. All species associated with human diphyllobothriid infections have marine or aquatic life cycles and transmission occurs via ingestion of undercooked fish.
2. Eggs are passed unembryonated in feces.
3. Under appropriate conditions, the eggs mature (approximately 18 to 20 days) and
4. yield oncospheres which develop into a coracidia.
5. After ingestion by a suitable crustacean (first intermediate host) the coracidia develop into procercoid larvae.
6. Procercoid larvae are released from the crustacean upon predation by the second intermediate host (usually a small fish) and migrate into the deeper tissues where they develop into a plerocercoid larvae (spargana), which is the infectious stage for the definitive host.
7. Because humans do not generally eat these small fish species raw, the second intermediate host probably does not represent an important source of human infection.
8. However, these small second intermediate hosts can be eaten by larger predator species that then serve as paratenic hosts.
9. In this case, the plerocercoid migrates to the musculature of the larger predator fish; humans (and other definitive host species) acquire the parasite via consumption of undercooked paratenic host fish.
10. In the definitive host, the plerocercoid develops into adult tapeworms in the small intestine. Adult diphyllobothriids attach to the intestinal mucosa by means of two bilateral groves (bothria) of their scolex.
11. Immature eggs are discharged from the proglottids (up to 1,000,000 eggs per day per worm) and are passed in the feces. Eggs appear in the feces 5 to 6 weeks after infection.
DIPHYLLOBOTHIRIUM LATUM PATHOGENESIS AND CLINICAL PRESENTATION
1. While most infections are asymptomatic,
2. complications include intestinal obstruction and
3. gall bladder disease caused by migration of proglottids.
4. weakness, weight loss, and other clinical features due to toxins released by the tapeworm.
5. Very occasionally a megaloblastic anaemia may develop due to the uptake of vitamin B12 by the tapeworm in competition with the host. This is more likely to occur when the tapeworm is situated in the upper part of the jejunum.
DIPHYLLOBOTHIRIUM LATUM LAB DIAGNOSIS
1. Diagnosis is made by the standard method of identification of eggs or segments of the tapeworm in a stool sample with a microscope.
2. Eggs: Single shell with operculum at one end and a knob on the other which are usually difficult to see
3. Many eggs are usually present in the faeces because they are constantly discharged through the uterine pore.
DIPHYLLOBOTHIRIUM LATUM TREATMENT
Praziquantel or niclosamide are used most often.
DIPHYLLOBOTHIRIUM LATUM PREVENTION AND CONTROL
1. Avoid eating raw or undercooked fish which may contain plerocercoids. Viable plerocercoids may also be found in pickled or smoked fish.
2. Killing the plerocercoids in fish by brine saturation or freezing at 10 °C for 24–48 hours and cooking of all fresh water fish.
3. Preventing the eggs reaching water bodies by providing adequate latrines, prohibit disposal of untreated sewage combined with health education.
4. Early laboratory diagnosis and treatment of the infected person
FASCIOLOPSIS BUSKI INTRODUCTION

Left: Fasciolopsis buski egg in an unstained wet mount.
Center: Adult fluke of F. buski next to a scale.
Right: Snail in the genus Hippeutis, an intermediate host for F. buski. (Credit: DPDx; Conchology, Inc., Mactan Island, Philippines)
The trematode Fasciolopsis buski, the largest (20 to 75 mm by 8 to 20 mm) intestinal fluke of humans causes faciolopsiasis.
FASCIOLOPSIS BUSKI DISTRIBUTION
Fasciolopsis is found in south and southeastern Asia.
FASCIOLOPSIS BUSKI TRANSMISSION AND LIFE CYCLE
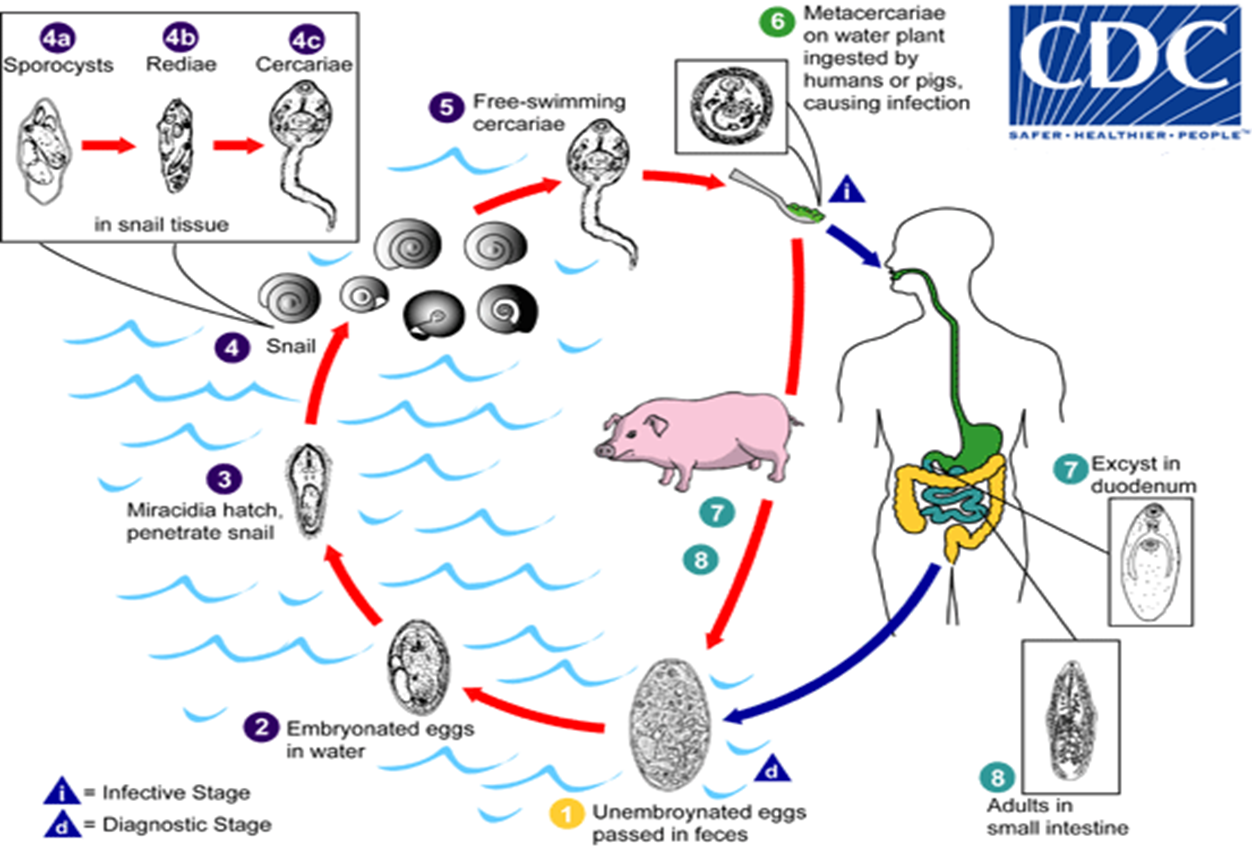
People become infected with Fasciolopsis when they eat raw or undercooked aquatic plants that have the organism encysted on them.
1. Immature eggs are discharged into the intestine and stool .
2. Eggs become embryonated in water ,
3. eggs release miracidia ,
4. which invade a suitable snail intermediate host . In the snail the parasites undergodevelopmental stages (sporocysts , rediae , and cercariae ).
5. The cercariae are released from the snail and
6. encyst as metacercariae on aquatic plants
7. The mammalian hosts become infected by ingesting metacercariae on the aquatic plants. After ingestion, the metacercariae excyst in the duodenum and attach to the intestinal wall.
8. Attached to the intestinal wall of the mammalian hosts (humans and pigs), they develop into adult flukes
FASCIOLOPSIS BUSKI PATHOGENESIS AND CLINICAL PRESENTATION
1. Many people do not have symptoms from Fasciolopsis infection.
2. However, abdominal pain and diarrhea can occur 1 or 2 months after infection.
3. With heavy infections Fasciolopsis flukes can cause intestinal obstruction, abdominal pain, nausea, vomiting, and fever.
4. Allergic reactions and swelling of the face, ascites and legs can also occur due to toxins produced by the flukes.
5. Plasma albumin levels may fall due to protein loss. There is usually a blood eosinophilia and slight macrocytic anaemia in heavily infected children can be fatal.
FASCIOLOPSIS BUSKI LAB DIAGNOSIS
1. Diagnosis is made by the standard method of identification of eggs of the fluke in a stool or vomit sample with a microscope.
2. Concentration techniques are rarely needed.
FASCIOLOPSIS BUSKI PREVENTION AND CONTROL
1. Treating water plants which may be infected using boiling water or cooking them before eating or teeth-peeling.
2. Providing latrines and health education to prevent eggs reaching the water (where humans are the main source of infection).
3. Avoiding the use of untreated human or pig faeces as fertilizer in cultivation ponds.
4. Identifying and destroying snail hosts and their habitats where this is feasible.
5. Early laboratory diagnosis and treatment of the infected persons and pigs
METAGONIMUS YOKOGAWAI INTRODUCTION
Metagonimus yokogawai, a minute intestinal fluke (and the smallest human fluke).
Figure A: Adult M. yokogawai, stained with carmine.
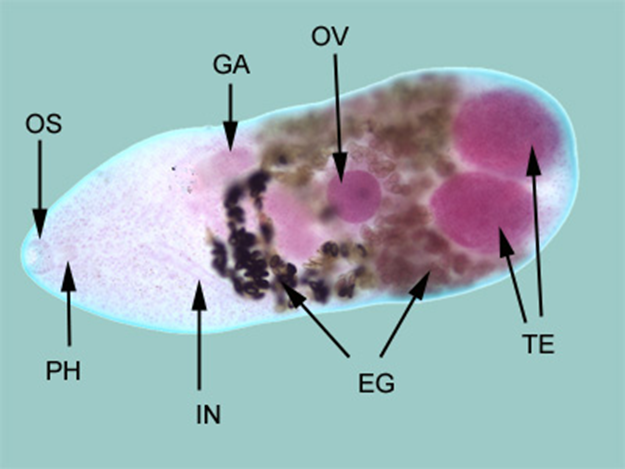
In this figure, the following structures are labeled:
oral sucker (OS), pharynx (PH),
intestine (IN), genitoacetabulum(GA),
ovary (OV), the large, paired testes (TE), and
eggs within the uterus (EG).
METAGONIMUS YOKOGAWAI INTRODUCTION
Metagonimus yokogawai, a minute intestinal fluke (and the smallest human fluke).
Figure A: Adult M. yokogawai, stained with carmine.
In this figure, the following structures are labeled:
oral sucker (OS), pharynx (PH),
intestine (IN), genitoacetabulum(GA),
ovary (OV), the large, paired testes (TE), and
eggs within the uterus (EG).
METAGONIMUS YOKOGAWAI DISTRIBUTION
Mostly the Far East, as well as Siberia, Manchuria, the Balkan states, Israel, and Spain.
METAGONIMUS YOKOGAWAI TRANSMISSION AND LIFE CYCLE
1. Adults release fully embryonated eggs each with a fully-developed miracidium, and eggs are passed in the host’s feces.
2. After ingestion by a suitable snail (first intermediate host), the eggs hatch and release miracidia which penetrate the snail’s intestine. Snails of the genus Semisulcospira are the most frequent intermediate host for Metagonimus yokogawai. The miracidia undergo several developmental stages in the snail, i.e. sporocysts 2a, rediae2b, and cercariae 2c. Many cercariae are produced from each redia.
3. The cercariae are released from the snail and
4. Adults release fully embryonated eggs each with a encyst as metacercariae in the tissues of a suitable fresh/brackish water fish (second intermediate host).
5. The definitive host becomes infected by ingesting undercooked or salted fish containing metacercariae.
6. After ingestion, the metacercariae excyst, attach to the mucosa of the small intestine and
7. mature into adults (measuring 1.0 mm to 2.5 mm by 0.4 mm to 0.75 mm).
8. In addition to humans, fish-eating mammals (e.g., cats and dogs) and birds can also be infected by M. yokogawai.
METAGONIMUS YOKOGAWAI PATHOGENESIS AND CLINICAL DIAGNOSIS
1. The main symptoms are diarrhea and colicky abdominal pain.
2. Migration of the eggs to extraintestinal sites (heart, brain) can occur, with resulting symptoms.
METAGONIMUS YOKOGAWAI LAB DIAGNOSIS
1. Diagnosis is made by the standard method of identification of eggs of the fluke in a stool sample with a microscope.
2. A concentration technique, such as the formol ether method may be necessary to detect the eggs.
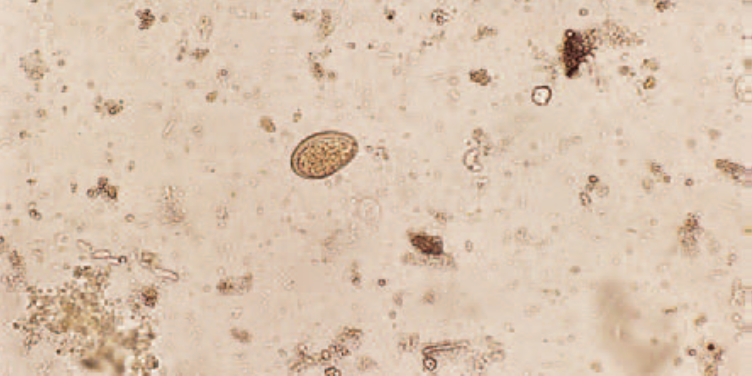
3. Egg of M.yokagawai ln a wet amount
4. Specific diagnosis is based on identification of the adult fluke evacuated after antihelminthic therapy, or found at autopsy.
HETEROPHYES HETEROPHYES INTRODUCTION
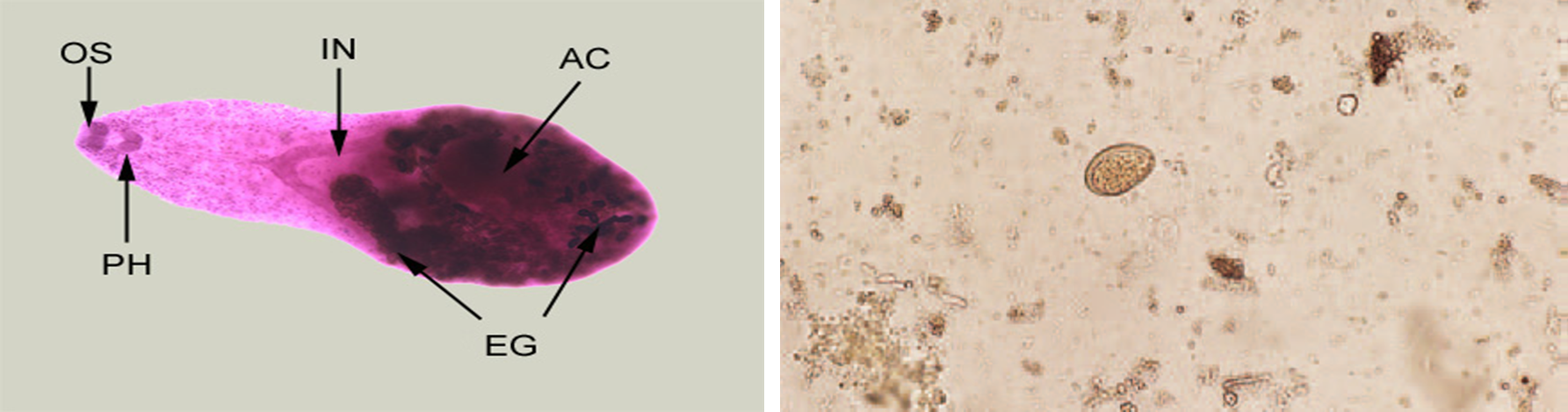
Left: Adult of H. heterophyes, stained with carmine.
oral sucker (OS), pharynx (PH), intestine (IN), ventral sucker, or acetabulum (AC), and eggs within the uterus (UT)
Right: Egg of H. heterophyes in a wet amount
- The trematode Heterophyes heterophyes, is a minute intestinal fluke, the adult measuring 1.0 to 1.7 mm by 0.3 to 0.4.
- Found in Egypt, the Middle East, and Far East.
HETEROPHYES HETEROPHYES TRANSMISSION AND LIFE CYCLE
1. Adults release embryonated eggs each with a fully-developed miracidium, and eggs are passed in the host’s feces.
2. After ingestion by a suitable snail (first intermediate host), the eggs hatch and release miracidia which penetrate the snail’s intestine. Genera Cerithidia and Pironella are important snail hosts in Asia and the Middle East respectively. The miracidia undergo several developmental stages in the snail, i.e. sporocysts 2a, rediae 2b, and cercariae 2c. Many cercariae are produced from each redia.
3. The cercariae are released from the snail and
4. encyst as metacercariae in the tissues of a suitable fresh/brackish water fish (second intermediate host).
5. The definitive host becomes infected by ingesting undercooked or salted fish containing metacercariae.
6. The metacercariae excyst, attach to the mucosa of the small intestine
7. and mature into adults and the cycle repeats.
8. In addition to humans, various fish-eating mammals (e.g., cats and dogs) and birds can be infected by Heterophyes heterophyes.
HETEROPHYES HETEROPHYES PATHOGENESIS AND CLINICAL PRESENTATIONS
1. The main symptoms are diarrhea and colicky abdominal pain.
2. Migration of the eggs to the heart, resulting in potentially fatal myocardial and valvular damage, has been reported from the Philippines.
3. Migration to other organs (e.g., brain) has also been reported.
HETEROPHYES HETEROPHYES LAB DIAGNOSIS
1. The diagnosis is based on the microscopic identification of eggs in the stool.
2. However, the eggs are indistinguishable from those of Metagonimus yokogawai and resemble those of Clonorchis and Opisthorchis.
Last modified: Saturday, 18 April 2026, 1:27 PM
Background Colour
Font Face
Font Kerning
Font Size
1
Image Visibility
Letter Spacing
0
Line Height
1.2
Link Highlight
Text Alignment
Text Colour