
Completion requirements
|
PARASITE HELIMINTHS |
LOCATION |
TRANSMISSION |
INFECTIVE STAGE |
MAIN DISEASE |
DIAGNOSTIC STAGE |
|
TREMATODES |
|||||
|
1. Schistosoma Species |
|||||
|
2. Fasciola Species |
|||||
|
3. Paragonimus westimani |
|||||
|
4. Opisthorchis (Clonorchis) species e.g O. fellineus, O. viverrini |
|||||
|
5. Dicrocoelium dendriticum |
|||||
|
FILARIAL AND OTHER TISSUE NEMATODES |
|||||
|
6. Wuchereria bancrofti, |
|||||
|
7. Brugia species, |
|||||
|
8. Loa loa, |
|||||
|
9. Onchocerca volvulus |
|||||
|
10. Drancunculus medinensis (Guinea worm), |
|||||
|
11. Echinococcus spp |
|||||
|
12. Trichinella species |
|||||
|
13. Toxocara canis |
|||||
|
14. Animal hookworms |
SCHISTOSOMA SPECIES INTRODUCTION

Images:
1. Left: Biomphalaria sp., the intermediate host for S. mansoni.
2. Center: Adults of S. mansoni. The thin female resides in the gynecophoral canal of the thicker male. The females (size ranges from 7–28 mm, depending on species)
3. Right: Bulinus sp., the intermediate host for S. haematobium and S. intercalatum
SCHISTOSOMA SPECIES DISTRIBUTION
1. Human schistosomiasis is found in areas bordering water bodies:
2. Schistosoma mansoni and S. haematobium
a. Distributed throughout Africa: including southern and sub-Saharan Africa esp in Sudan and Egypt.
b. South America: Including Brazil, Suriname, and Venezuela.
c. Caribbean (risk is very low): Dominican Republic, Guadeloupe, Martinique, and Saint Lucia.
3. S. japonicum: Found in Indonesia and parts of China and S. East Asia.
4. S. mekongi: Found in Cambodia and Laos.
5. S. intercalatum: Found in parts of Central and West Africa.
SCHISTOSOMA SPECIES TRANSMISSION & LIFE CYCLE
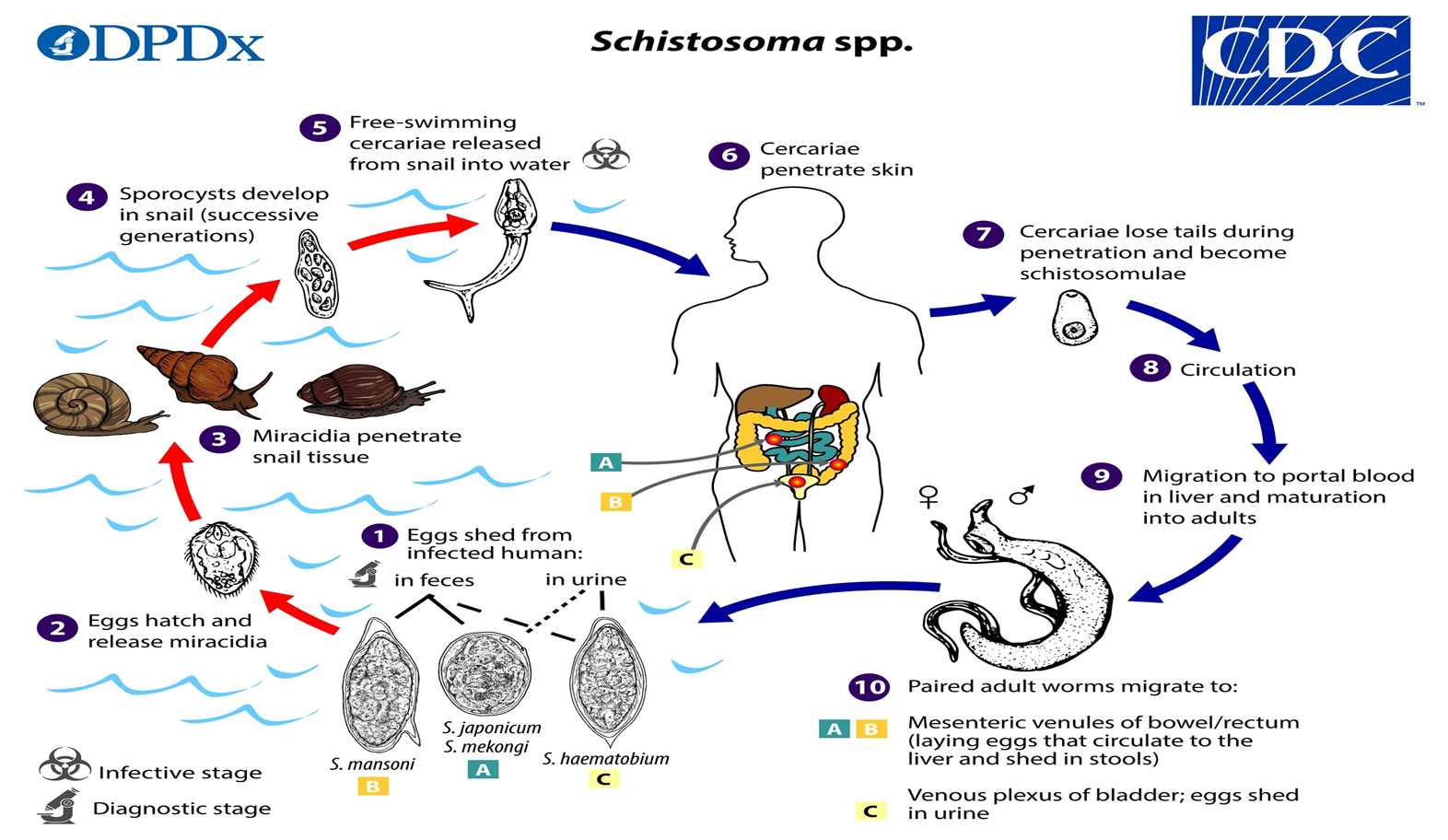
1. Schistosoma eggs are eliminated with feces or urine, depending on species.
2. Under appropriate conditions the eggs hatch and release miracidia
3. which swim and penetrate specific snail intermediate hosts.
4. The stages in the snail include two generations of sporocysts
5. and the production of cercariae.
6. Upon release from the snail, the infective cercariae swim, penetrate the skin of the human host,
7. and shed their forked tails, becoming schistosomulae.
8. The schistosomulae migrate via venous circulation to lungs, then to the heart, and then develop in the liver,
9. exiting the liver via the portal vein system when mature.
10. Male and female adult worms copulate and reside in the mesenteric venules, the location of which varies by species (with some exceptions).
The eggs are moved progressively toward the lumen of the intestine (S. mansoni,S. japonicum, S. mekongi, S. intercalatum/guineensis) and of the bladder and ureters (S. haematobium), and are eliminated with feces or urine, respectively.
SCHISTOSOMA SPECIES PATHOGENESIS AND CLINICAL PRESENTATION
1. Pathology associated with S. mansoni and S. japonicum schistosomiasis includes various hepatic complications from inflammation and granulomatous reactions, and occasional embolic egg granulomas in brain or spinal cord.
2. Pathology of S. haematobium schistosomiasis includes hematuria, scarring, calcification, squamous cell carcinoma, and occasional embolic egg granulomas in brain or spinal cord.
3. Many infections are asymptomatic. Symptoms of schistosomiasis are not caused by the worms themselves but by the body’s reaction to the eggs.
4. A local cutaneous hypersensitivity reaction following skin penetration by cercariae may occur and appears as small, itchy maculopapular lesions. Acute schistosomiasis (Katayama fever) is a systemic hypersensitivity reaction that may occur weeks after the initial infection, especially by S. mansoni and S. japonicum.
5. Manifestations include systemic symptoms/signs including fever, cough, abdominal pain, diarrhea, hepatosplenomegaly, and eosinophilia.
6. Occasionally, Schistosoma infections may lead to central nervous system lesions. Cerebral granulomatous disease may be caused by ectopic S. japonicum eggs in the brain, and granulomatous lesions around ectopic eggs in the spinal cord may occur in S. mansoni and S. haematobium infections. Chronic infection may cause granulomatous reactions and fibrosis in the affected organs (e.g., liver, bladder and spleen) with associated signs/symptoms.
7. Rarely, eggs are found in the brain or spinal cord and can cause seizures, paralysis, or spinal cord inflammation.
SCHISTOSOMA SPECIES LAB DIAGNOSIS
1. Careful review of travel and residence history is critical – endemicity of sub-Saharan Africa.
2. Examination of stool and/or urine for ova is the primary method of diagnosis for suspected schistosome infections.
3. The eggs are shed intermittently and in low amounts in light-intensity infections. Thus, may need concentration methods.
4. Serologic testing for anti-schistosomal antibody is indicated for diagnosis of travelers or immigrants from endemic.
5. An antigen test has been developed that can detect active infection based on the presence of schistosomal antigen, still under evaluation.
SCHISTOSOMA SPECIES TREATMENT
1. Safe and effective medication is available for treatment of both urinary and intestinal schistosomiasis.
2. Praziquantel, a prescription medication, is taken for 1-2 days to treat infections caused by all schistosome species.
SCHISTOSOMA SPECIES PREVENTION AND CONTROL
1. No Schistosomiasis infection vaccination available.
2. Avoid swimming or wading in freshwater when you are in countries in which schistosomiasis occurs. Swimming in the ocean and in chlorinated swimming pools is safe.
3. Vigorous towel drying after an accidental NOT RELIABLE
Control efforts usually focus on:
4. Reducing the number of infections in people and/or early lab diagnosis and Mass drug administration
5. Eliminating the snails that are required to maintain the parasite’s life cycle.
FASCIOLA SPECIES INTRODUCTION

Images:
1. Left: Fasciola hepatica egg in an unstained wet mount (400x magnification), and measure 130–150 μm by 60–90 µm.
2. Center: Adult Fasciola hepatica fluke stained with carmine (30mm x 13mm).
3. Right: Fossaria bulamoides, a snail host for F. hepatica in the western United States.
1. Fascioliasis occurs in many areas of the world and usually is caused by F. hepatica, which is a common liver fluke of sheep and cattle.
2. It is found in parts of Latin America, the Caribbean, Europe, the Middle East, Africa, Asia, and Oceania.
3. Fasciola gigantica is found in fewer geographic regions. Human cases have been reported in the tropics, in parts of Africa and Asia, and also in Hawaii.
4. F. gigantica: up to 75 mm by 15 mm), which are primarily found in domestic and wild ruminants (their main definitive hosts) but also are causal agents of fascioliasis in humans.
5. Although F. hepatica and F. gigantica are distinct species, “intermediate forms” that are thought to represent hybrids of the two species EXISTS.
FASCIOLA SPECIES TRANSMISSION AND LIFE CYCLE
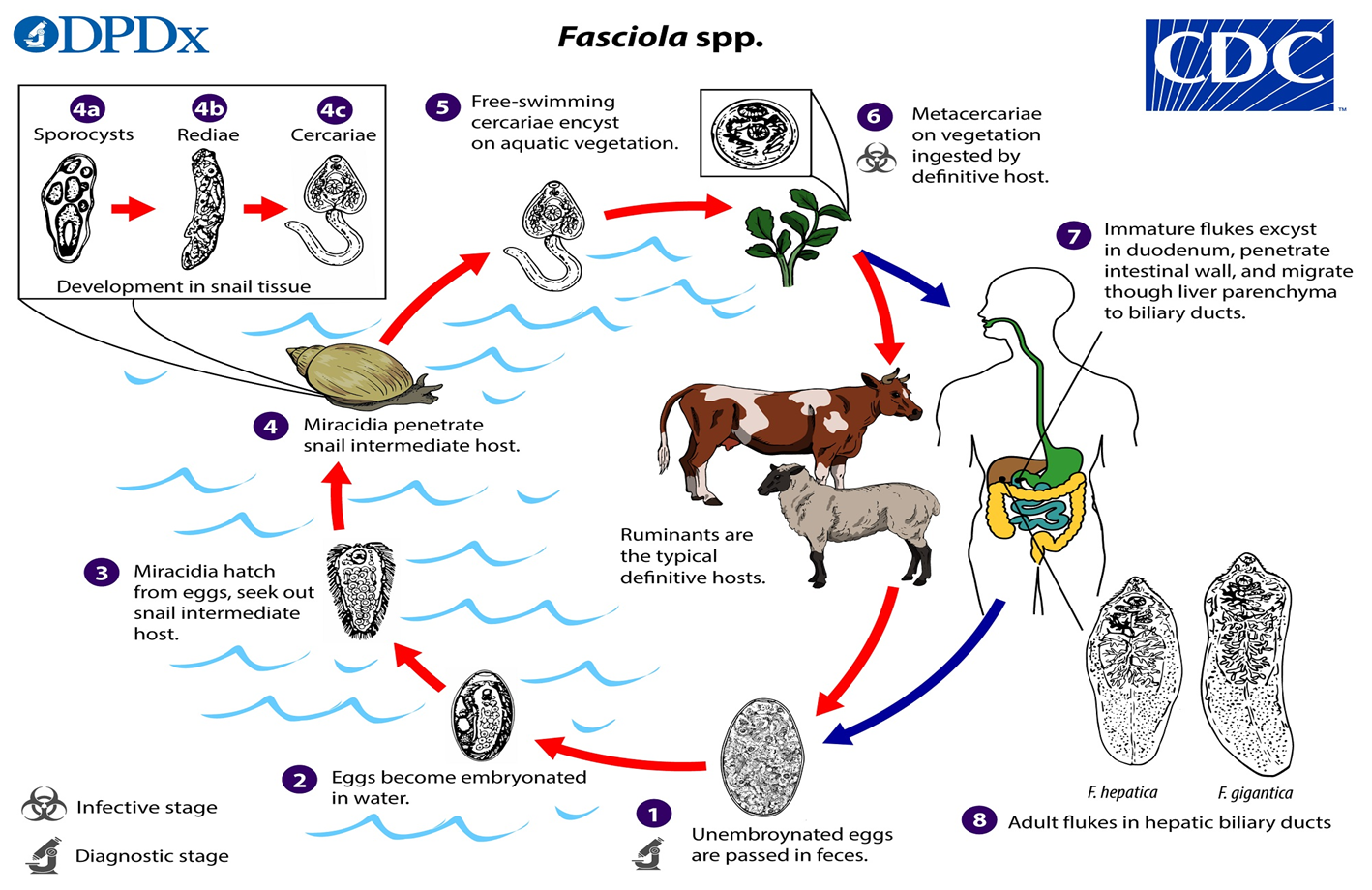
1. Immature eggs are discharged in the biliary ducts and passed in the stool.
2. Eggs become embryonated in freshwater over ~2 weeks;
3. embryonated eggs release miracidia,
4. which invade a suitable snail intermediate host. In the snail, the parasites undergo several developmental stages (sporocysts, rediae, and cercariae).
5. The cercariae are released from the snail and encyst as metacercariae on aquatic vegetation or other substrates.
6. Humans and other mammals become infected by ingesting metacercariae-contaminated vegetation (e.g., watercress).
7. After ingestion, the metacercariae excyst in the duodenumand penetrate through the intestinal wall into the peritoneal cavity.
8. The immature flukes then migrate through the liver parenchyma into biliary ducts, where they mature into adult flukes and produce eggs.
In humans, maturation from metacercariae into adult flukes usually takes about 3–4 months; development of F. gigantica may take somewhat longer than F. hepatica.
FASCIOLA SPECIES PATHOGENESIS AND CLINICAL PRESENTATION
Fasciola spp. infection in humans may or may not be associated with symptoms or other clinical manifestations, during acute and chronic phases.
During the Acute Phase: the early phase of the infection, also, known as migratory, invasive, hepatic, parenchymal, or larval phase, can be associated with:
1. Inflammation, tissue destruction, and toxic/allergic reactions.
2. Nonspecific symptoms/signs (e.g., abdominal pain, nausea, vomiting, hepatomegaly, malaise, fever, cough) and laboratory abnormalities (e.g., peripheral eosinophilia, elevated transaminase levels) may develop.
3. Occasionally, larval flukes migrate to ectopic sites, such as the lungs, subcutaneous tissue, pancreas, genitourinary tract, eyes, or brain.
During the Chronic Phase of the infection (also referred to as the biliary or adult phase), clinical manifestations, if any, may develop months to years post exposure and include:
1. Inflammation or blockage of bile ducts or the gallbladder (e.g., cholangitis, cholecystitis), which can be intermittent.
2. Inflammation of the pancreas may also occur.
FASCIOLA SPECIES LAB DIAGNOSIS
1. The standard way to be sure a person is infected with Fasciola is by finding Fasciola eggs in stool (fecal) specimens examined under a microscope.
2. Sometimes eggs are found by examining duodenal contents or bile.
3. Early and chronic infection has to be diagnosed using tests that detect antibodies (an immune response) to the parasite.
FASCIOLA SPECIES TREATMENT
The drug of choice is triclabendazole. The drug is given by mouth, usually in two doses. Most people respond well to the treatment.
FASCIOLA SPECIES PREVENTION AND CONTROL
1. No Fasciola infection vaccine is available.
2. Strict control of the growth and sale of watercress and other edible water plants is important.
3. Individual people can protect themselves by not eating raw watercress and other water plants, especially from Fasciola-endemic grazing areas.
4. As always, travelers to areas with poor sanitation should avoid food and water that might be contaminated (tainted).
5. Vegetables grown in fields that might have been irrigated with polluted water should be thoroughly cooked, as should viscera from potentially infected animals.
PARAGONIMUS WESTERMANI INTRODUCTION
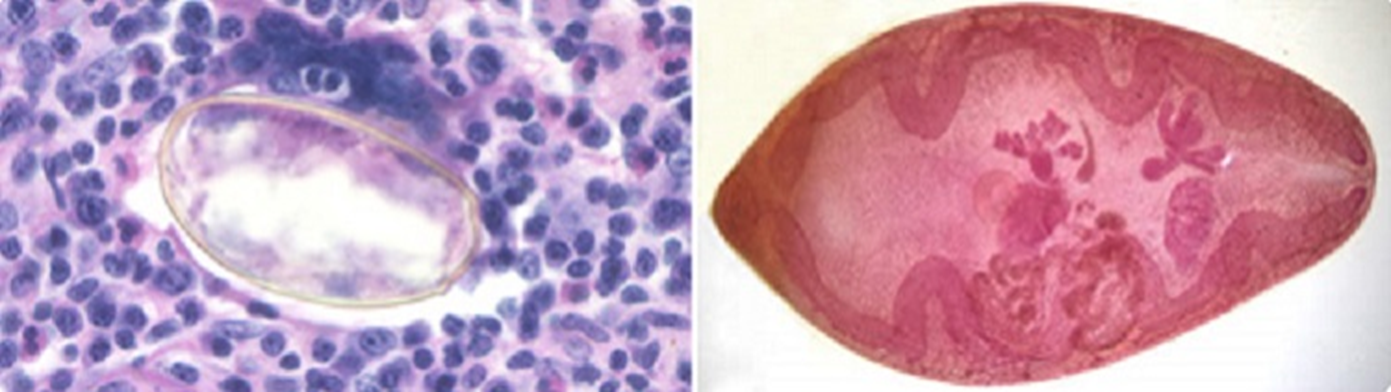
Images:
1. Left: Eggs of Paragonimus sp. taken from a lung biopsy stained with hematoxylin and eosin (H&E). These eggs measured 80-90 µm by 40-45 µm. The species was not identified in this case.
2. Right: P. westermani adult, this approximately 1cm long fluke is viewed under magnification.
1. More than 30 species of trematodes (flukes) of the genus Paragonimus have been reported which infect animals and humans.
2. Paragonimus is a lung fluke (flatworm) that infects the lungs of humans after eating an infected raw or undercooked crab or crayfish.
3. Among the more than 10 species reported to infect humans, the most common is P. westermani, the oriental lung fluke.
4. Less frequent, but more serious cases of paragonimiasis occur when the parasite travels to the central nervous system.
5. It occurs primarily in Asia including China, the Philippines, Japan, Vietnam, South Korea, Taiwan, and Thailand. P. africanus causes infection in Africa, and P. mexicanus in Central and South America.
PARAGONIMUS WESTERMANI TRANSMISSION AND LIFE CYCLE
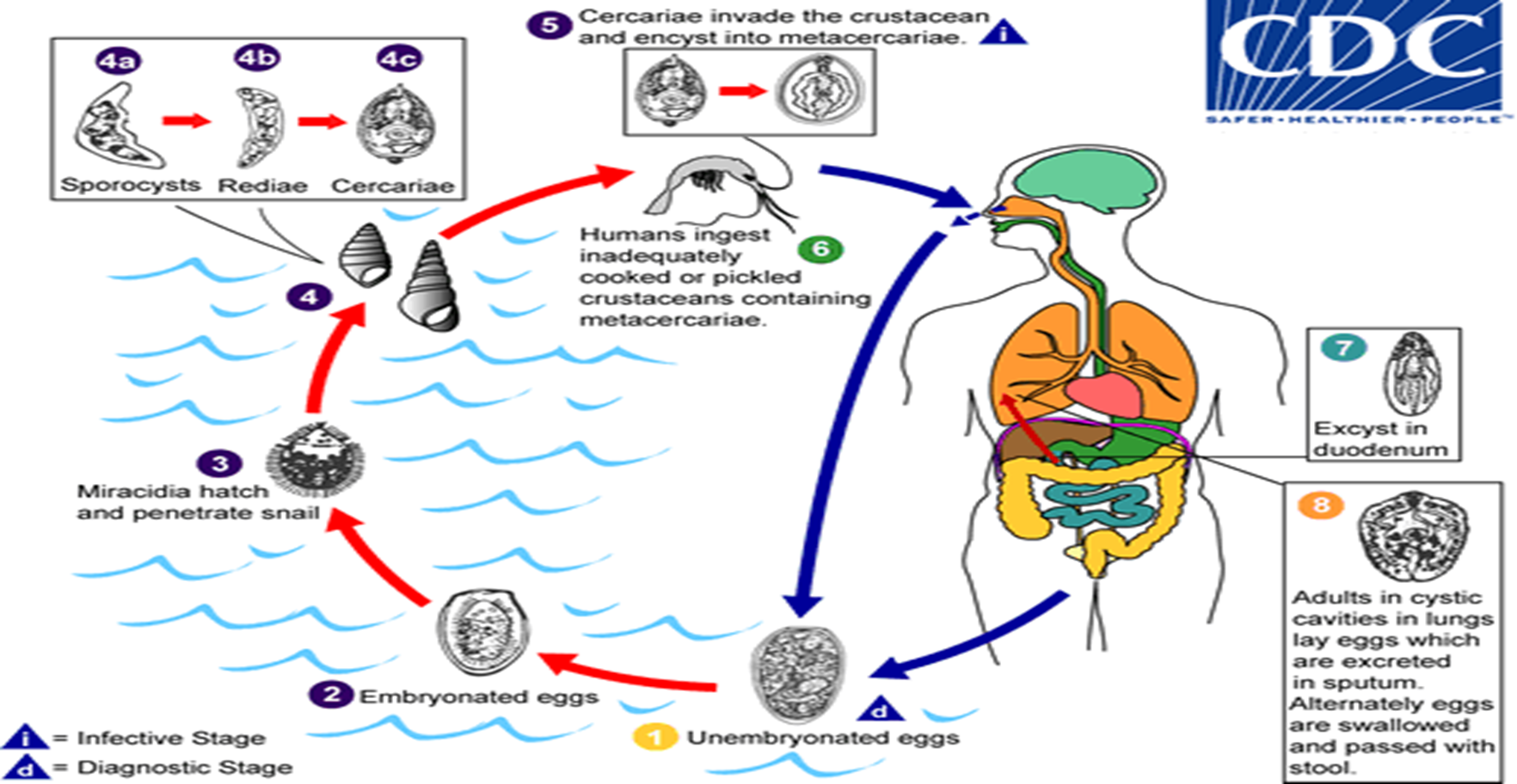
1. The eggs are excreted unembryonated in the sputum, or alternately they are swallowed and passed with stool.
2. In the external environment, the eggs become embryonated,
3. and miracidia hatch and seek the first intermediate host, a snail, and penetrate its soft tissues.
4. Miracidia go through several developmental stages inside the snail: sporocysts, rediae, with the latter giving rise to many cercariae, which emerge from the snail.
5. The cercariae invade the second intermediate host, a crustacean such as a crab or crayfish, where they encyst and become metacercariae. This is the infective stage for the mammalian host.
6. Human infection with P. westermani occurs by eating inadequately cooked or pickled crab or crayfish that harbor metacercariae of the parasite.
7. The metacercariae excyst in the duodenum, penetrate through the intestinal wall into the peritoneal cavity,
8. then through the abdominal wall and diaphragm into the lungs, where they become encapsulated and develop into adults. (7.5 to 12 mm by 4 to 6 mm).
The worms can also reach other organs and tissues, such as the brain and striated muscles, respectively. However, when this takes place completion of the life cycles is not achieved, because the eggs laid cannot exit these sites. Time from infection to oviposition is 65 to 90 days. Infections may persist for 20 years in humans. Animals such as pigs, dogs, and a variety of feline species can also harbor P. westermani.
PARAGONIMUS WESTERMANI PATHOGENESIS AND CLINICAL PRESENTATION
1. The acute phase (invasion and migration) may be marked by diarrhea, abdominal pain, fever, cough, urticaria, hepatosplenomegaly, pulmonary abnormalities, and eosinophilia.
2. During the chronic phase, pulmonary manifestations include cough, expectoration of discolored sputum, hemoptysis, and chest radiographic abnormalities.
3. Extra-pulmonary locations of the adult worms result in more severe manifestations, especially when the brain is involved.
PARAGONIMUS WESTERMANI LAB DIAGNOSIS
1. The infection is usually diagnosed by identification of Paragonimus eggs in sputum.
2. The eggs are sometimes found in stool samples (coughed-up eggs are swallowed).
3. A tissue biopsy is sometimes performed to look for eggs in a tissue specimen.
4. Specific and sensitive antibody tests based on P. westermani antigens are available through CDC, and serologic tests using a variety of techniques are available through commercial laboratories.
PARAGONIMUS WESTERMANI TREATMENT
1. Praziquantel is the drug of choice: adult or pediatric dosage, 25 mg/kg given orally three times per day for 2 consecutive days.
2. For cerebral disease, a short course of corticosteroids may be given with the praziquantel to help reduce the inflammatory response around dying flukes.
3. Alternative: Triclabendazole, 2 doses of 10 mg/kg given 12 hours apart in patients 6 years of age and older.
PARAGONIMUS WESTERMANI PREVENTION AND CONTROL
1. Never eat raw freshwater crabs or crayfish.
2. Cook crabs and crayfish for to at least 145°F (~63°C).
3. Travelers should be advised to avoid traditional meals containing undercooked freshwater crustaceans.
OPISTHORCHIS SPECIES INTRODUCTION

Images:
1. Left: Adult of O. felineus.
2. Right: A large group of fish.
1. Opisthorchis species are liver fluke parasites (trematodes or worms).
2. Opisthorchis viverrini is known as the Southeast Asian liver fluke and
3. O. felineus is known as the cat liver fluke.
4. O. viverrini is found mainly in northeast Thailand, Laos, Cambodia, and central and southern Vietnam.
5. O. felineus is found mainly in Italy, Germany, Belarus, Russia, Kazakhstan, and Ukraine.
6. Travelers to Asia or Europe who consume raw or undercooked fish are at risk for liver fluke infection.
OPISTHORCHIS SPECIES TRANSMISSION AND LIFE CYCLE
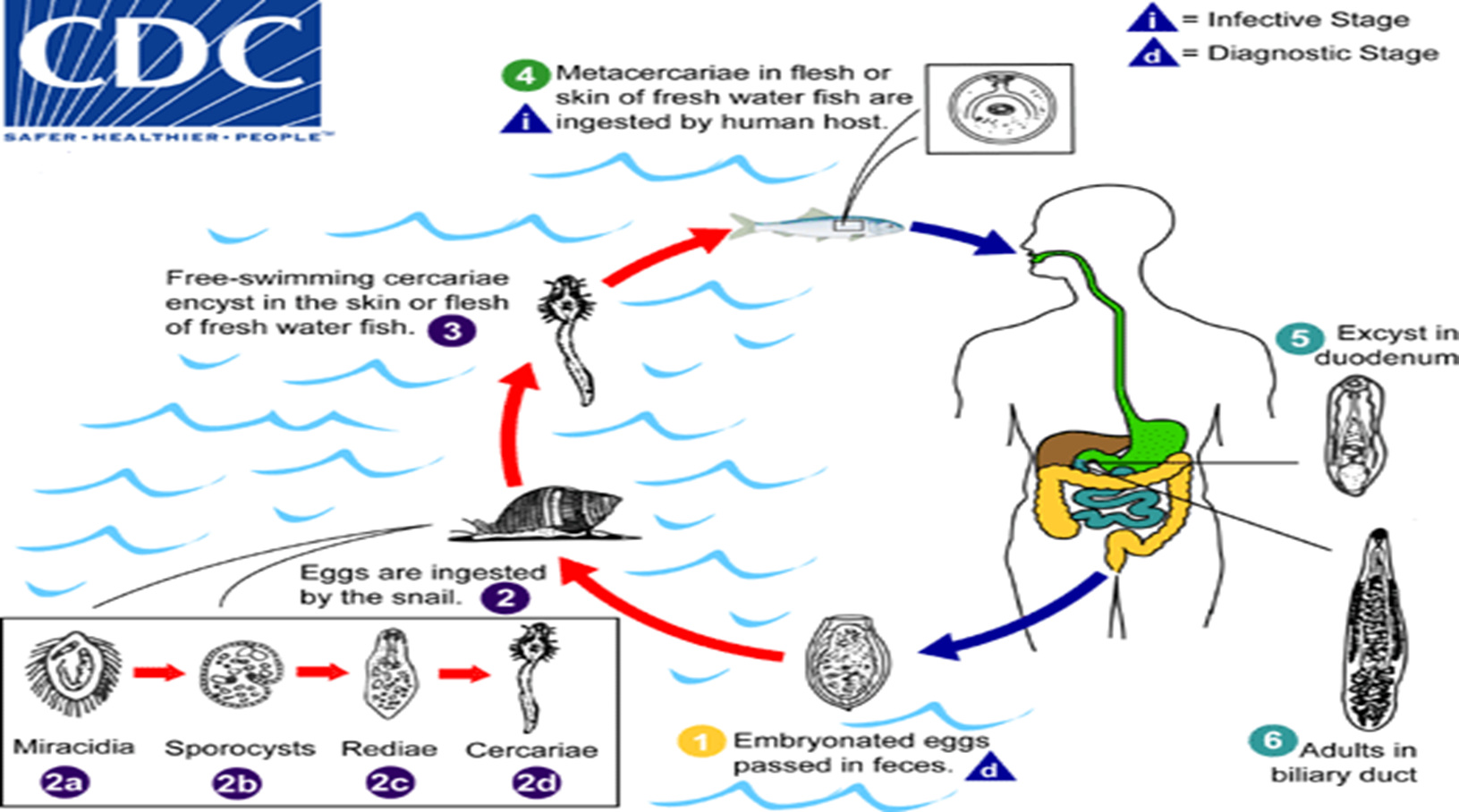
1. The adult flukes deposit fully developed eggs that are passed in the feces.
2. After ingestion by a suitable snail (first intermediate host) the eggs release miracidia 2a , which undergo in the snail several developmental stages (sporocysts 2b, rediae 2c, cercariae 2d ).
3. Cercariae are released from the snail and
4. And penetrate freshwater fish (second intermediate host), encysting as metacercariae in the muscles or under the scales.
5. The mammalian definitive host (cats, dogs, and various fish-eating mammals including humans) become infected by ingesting undercooked fish containing metacercariae. After ingestion, the metacercariae excyst in the duodenum
6. And ascend through the ampulla of Vater into the biliary ducts, where they attach and develop into adults, which lay eggs after 3 to 4 weeks.
The adult flukes (O. viverrini: 5 mm to 10 mm by 1 mm to 2 mm; O. felineus: 7 mm to 12 mm by 2 mm to 3 mm) reside in the biliary and pancreatic ducts of the mammalian host, where they attach to the mucosa.
OPISTHORCHIS SPECIES PATHOGENESIS AND CLINICAL PRESENTATION
Most pathologic manifestations result from inflammation and intermittent obstruction of the biliary ducts. Most infections are asymptomatic.
1. In mild cases, manifestations include dyspepsia, abdominal pain, diarrhea, or constipation.
2. With infections of longer duration, the symptoms can be more severe, and hepatomegaly and malnutrition may be present.
3. In rare cases, cholangitis, cholecystitis, and chlolangiocarcinoma may develop.
4. In addition, infections due to Opisthorchis felineus may present an acute phase resembling Katayama fever (schistosomiasis), with fever, facial edema, lymphadenopathy, arthralgias, rash, and eosinophilia.
5. Chronic forms of Opisthorchis felineus infections present the same manifestations as Opisthorchis viverrini, with in addition involvement of the pancreatic ducts.
6. Infections are not known to last longer than 25–30 years, the life span of the parasite.
OPISTHORCHIS SPECIES TREATMENT
Praziquantel or albendazole are the drugs of choice to treat Opisthorchis infection.
OPISTHORCHIS SPECIES PREVENTION AND CONTROL
1. The FDA recommends the following for fish preparation or storage to kill any parasites.
2. Cooking
a. Cook fish adequately (to an internal temperature of at least 145° F [~63° C]).
3. Freezing (Fish)
a. At -4°F (-20°C) or below for at least 7 days (total time); or
b. At -31°F (-35°C) or below until solid, and storing at -31°F (-35°C) or below for at least 15 hours; or
c. At -31°F (-35°C) or below until solid and storing at -4°F (-20°C) or below for at least 24 hours.
DICROCOELIUM SPECIES INTRODUCTION

Images:
1. Left: Adultof D. dendriticum, stained with carmine. Structures illustrated: oral sucker (OS), acetabulum (AC), uterus (UT), testes (TE), and vitelline glands (VT).
2. Right: Egg of Dicrocoelium dendriticum in an unstained wet mount of stool. Image courtesy of Dr. Juan Cuadros González.
1. The trematode Dicrocoelium dendriticum, the lanceolate fluke or lancet fluke, is a common parasite of ruminants but humans can be accidental definitive hosts.
2. Another species, D. hospes, is responsible for human infections in West Africa.
3. Most of the known clinical cases have occurred in North Africa and the Middle East.
4. D. hospes is endemic in sub-Saharan West Africa; cases have been documented in Ghana, Senegal, Sierra Leone, and Mali.
DICROCOELIUM SPECIES TRANSMISSION AND LIFE CYCLE
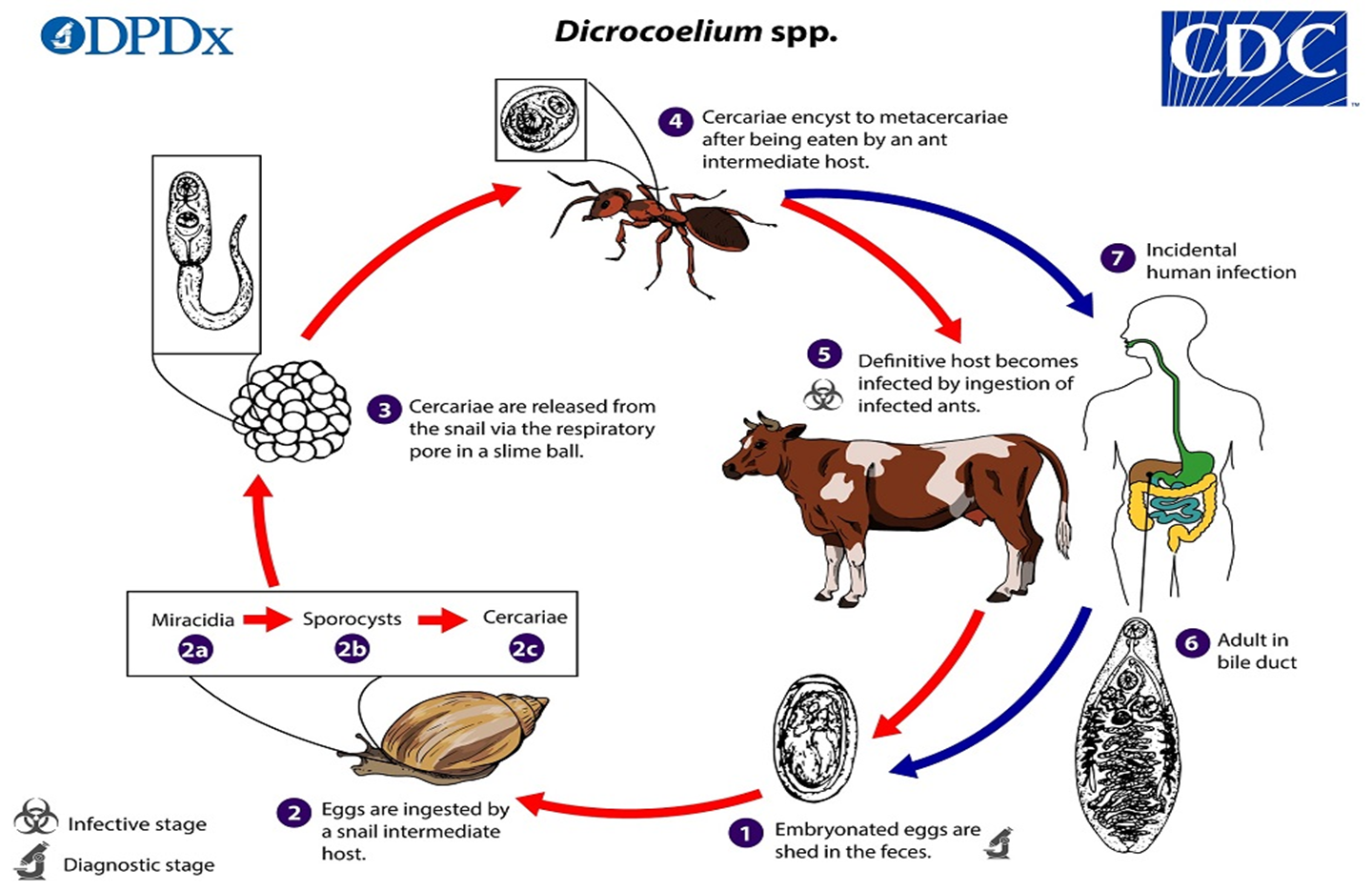
1. Embryonated eggs containing miracidia are shed in feces of definitive hosts, which are typically ruminants.
2. The eggs are then ingested by the first intermediate host (snail such as those in the genera Cochlicopa). When the miracidia hatch 2a, they migrate through the gut wall and settle into the adjacent vascular connective tissue, where they become mother sporocysts 2b. The sporocysts migrate to the digestive gland where they give rise to several daughter sporocysts. Inside each daughter sporocyst, cercariae 2c are produced. Cercariae migrate to the respiration chamber where they are shed in slime ball from the snail.
3. After a slime ball is ingested by the second intermediate host (ant especially members of the genus Formica), the cercariae become free in the intestine and
4. migrate to the hemocoel where they become metacercariae.
5. When the infected ant is eaten by a suitable definitive host, the metacercariae excyst in the small intestine.
6. The worms migrate to the bile duct where they mature into adults.
7. Humans can serve as definitive hosts after ingesting infected ants (e.g. on contaminated food items).
DICROCOELIUM SPECIES CLINICAL PRESENTATION
1. Most infections involve low numbers of flukes and are not associated with overt symptoms.
2. In more intense infections, symptoms may include cholecystitis, liver abscesses, and generalized gastrointestinal/abdominal distress.
3. Occasional cases involving flukes in subcutaneous masses have been reported.
DICROCOELIUM SPECIES LAB DIAGNOSIS
1. Diagnosis is based on microscopic identification of eggs in the stool, duodenal, and/or bile fluid.
2. Note that eggs may be detected in stool following consumption of liver infected with adult flukes;
3. Additional specimens should be collected to distinguish this spurious passage from a true infection.
4. Adult flukes are rarely recovered.
WUCHERERIA BANCROFTI, BRUGIA MALAYI, BRUGIA TIMORI (LYMPHATIC FILARIASIS)
LYMPHATIC FILARIASIS INTRODUCTION

LYMPHATIC FILARIASIS INTRODUCTION
Images of adults of:
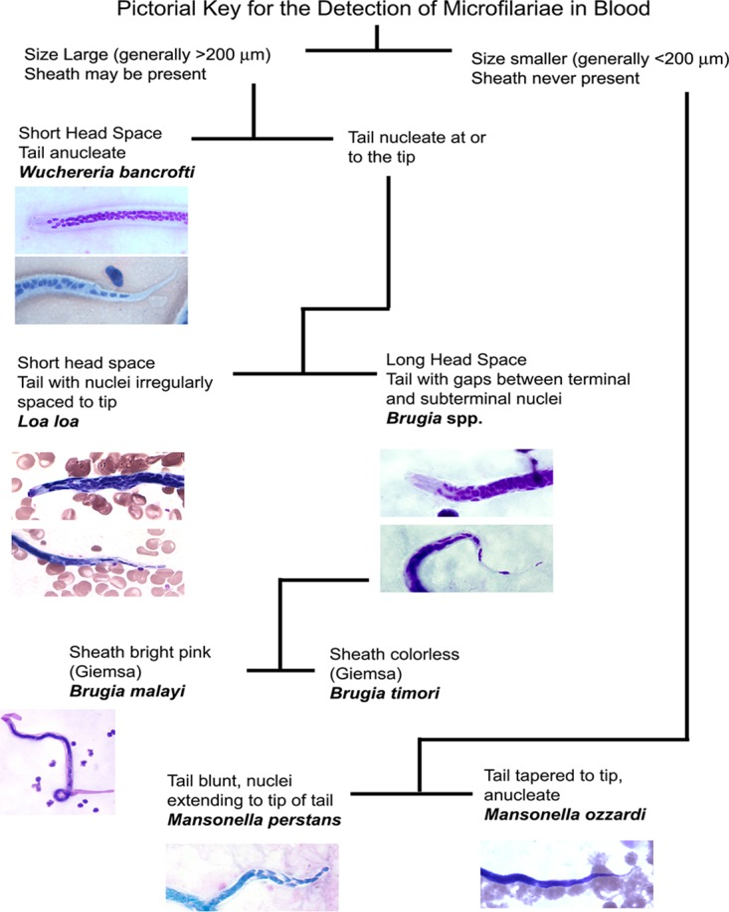
1. Figure Left: Microfilaria of W. bancrofti in a thick blood smear stained with Giemsa. Image courtesy of the Oregon State Public Health Laboratory. Adults of Wuchereria bancrofti are long and threadlike.
i. The males measure up to 40 mm long and females are 80—100 mm long. Adults are found primarily in lymphatic vessels, less commonly in blood vessels.
2. Figure Center: Microfilaria of B. malayi in a thick blood smear, stained with Giemsa. Microfilariae of Brugia malayi are sheathed and in stained blood smears measure 175—230 µm. In 2% formalin they are longer, measuring 240—300 µm. The tail is tapered, with a significant gap between the terminal and subterminal nuclei. Microfilaria circulate in the blood.
3. Figure Right: Microfilaria of B. timori in a thick blood smear, stained with Giemsa and captured at 500x oil magnification. Image from a courtesy of Dr. Thomas C. Orihel, Tulane University, New Orleans, LA.
4. W. bancrofti is currently endemic throughout Sub-Saharan Africa (excluding the southern portion of the continent), Madagascar, several Western Pacific Island nations and territories and parts of the Caribbean. occurs sporadically in S. America, India, and S. East Asia.
5. Brugia spp. associated with LF are more geographically limited and occur only in S. E. Asia.
6. Brugia timori is restricted to the Lesser Sunda Islands of Indonesia.
LYMPHATIC FILARIASIS LIFE CYCLE
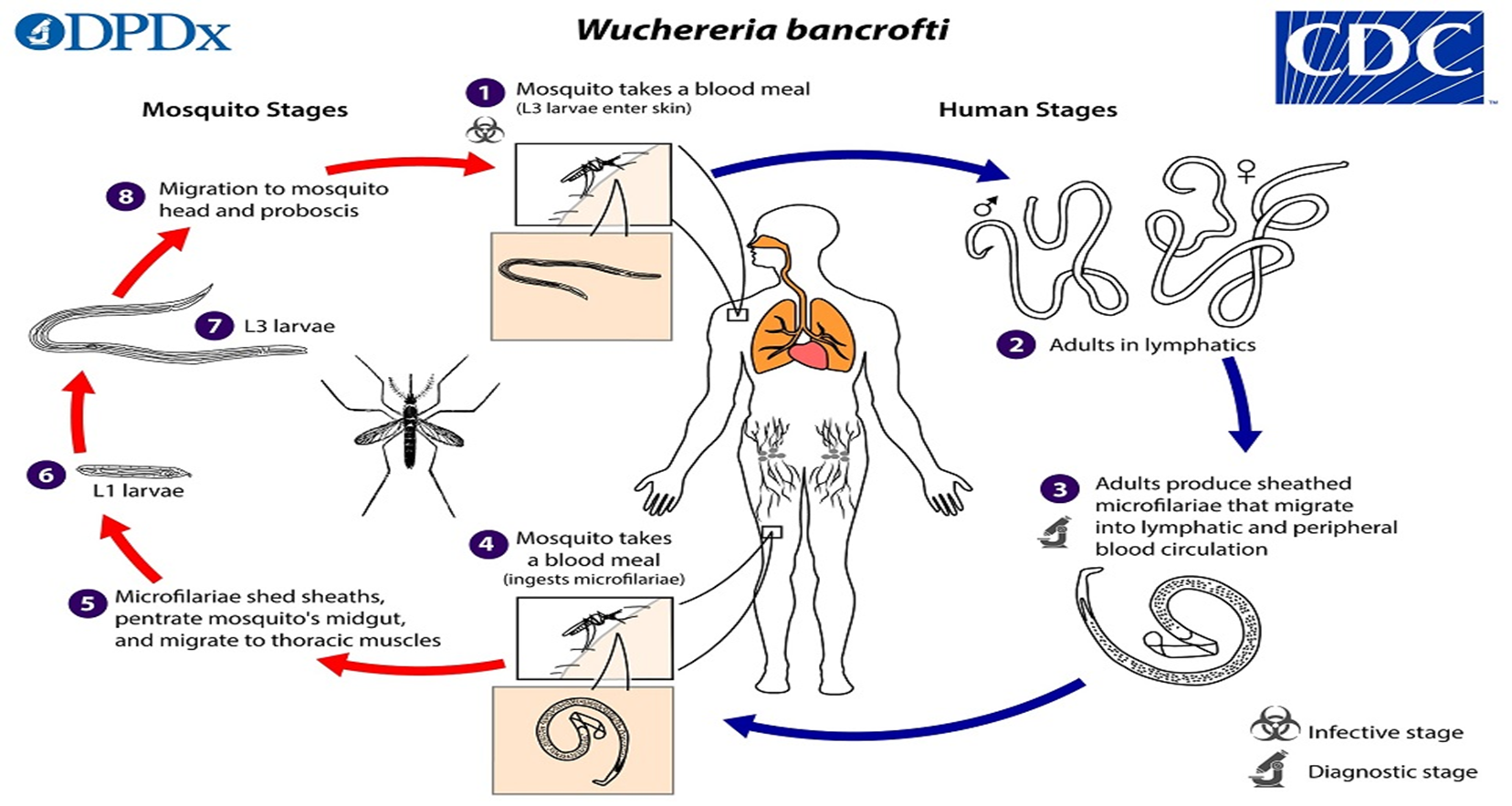
1. During a blood meal, an infected mosquito introduces third-stage filarial larvae onto the skin of the human host, where they penetrate into the bite wound.
2. They develop in adults that commonly reside in the lymphatics. Adults produce microfilariae which show nocturnal periodicity, except the South Pacific microfilariae which have the absence of marked periodicity.
3. The microfilariae migrate into lymph and blood channels moving actively through lymph and blood.
4. A mosquito ingests the microfilariae during a blood meal.
5. After ingestion, the microfilariae lose their sheaths and some of them work their way through the wall of the proventriculus and cardiac portion of the mosquito’s midgut and reach the thoracic muscles.
6. There the microfilariae develop into first-stage larvae.
7. and subsequently into third-stage infective larvae.
8. The third-stage infective larvae migrate through the hemocoel to the mosquito’s prosbocis, and can infect another human when the mosquito takes a blood meal.
W. bancrofti is transmitted by many different mosquito genera/species, depending on geographical distribution.
Among them are Aedes spp., Anopheles spp., Culex spp., Mansonia spp., and Coquillettida juxtamansonia.
Brugia spp follow the same/similar life cycle with the typical vector for Brugia spp. filariasis being mosquito species in the genera Mansonia and Aedes.
LYMPHATIC FILARIASIS PATHOGENESIS AND CLINICAL PRESENTATION

Patient with lymphedema (CDC Photo)
While severe manifestations do not develop in the majority of infections, LF is a potentially highly disfiguring and disabling disease.
1. The most prominent clinical feature is the development of severe lymphedema of the limbs (“elephantiasis”) and occasionally genitalia (hydrocele) due to dysfunction of lymphatic vessels.
2. Affected limbs become grossly swollen; the skin may become thick and pitted, and secondary infection are frequent due to lymphatic dysfunction.
3. Scrotal hydrocele is also seen in some infected males. Lymphangitis, lymphadenopathy, and eosinophilia may accompany infection in the early stages.
4. Patients are also vulnerable to secondary bacterial infections
5. A chronic syndrome called “tropical pulmonary eosinophilia” has been associated with W. bancrofti and B. malayi infections, involving eosinophilic pulmonary infiltrate, peripheral hypereosinophilia, wheezing, chest pain, splenomegaly, and bloody sputum. This has most frequently been documented in South and Southeast Asia.
LYMPHATIC FILARIASIS LAB DIAGNOSIS
1. The standard method for diagnosing active infection is by microscopic examination of a blood smear.
2. Blood collection should be done at night (nocturnal periodicity) to coincide with the appearance of the microfilariae, and a thick smear should be made and stained with Giemsa.
3. For increased sensitivity, concentration (e.g Microhaematocrit tube, Tube centrifugation lyzed venous blood, techniques).
4. Serologic techniques provide an alternative to microscopic for the active infections.
5. Because lymphedema may develop many years after infection, lab tests are most likely to be negative with these patients.
LYMPHATIC FILARIASIS TREATMENT
1. Diethylcarbamazine (DEC) is the drug of choice for the active lymphatic filariasis.
2. DEC should not be administered to patients who may also have onchocerciasis as DEC can worsen onchocercal eye disease.
3. In settings where onchoceriasis is present, Ivermectin is the drug of choice to treat LF.
4. People with lymphedema and elephantiasis are unlikely to benefit from DEC.
LYMPHATIC FILARIASIS PREVENTION AND CONTROL
1. In an area with lymphatic filariasis:
2. At night
a. Sleep in an air-conditioned room or
b. Sleep under a mosquito net
3. Between dusk and dawn
a. Wear long sleeves and trousers and
b. Use mosquito repellent on exposed skin.
4. Regular mass drug administration
LOA LOA INTRODUCTION

Loa loa, a filarid nematode commonly referred to as the African eye worm that cause loiasis disease
1. Left: Microfilaria of L. loa in a thin blood smear, stained with Giemsa.
2. Right: Chrysops silacea feeding on a volunteer. (Credit: DPDx)
3. The female worms measure 40 to 70 mm in length and 0.5 mm in diameter,
4. while the males measure 30 to 34 mm in length and 0.35 to 0.43 mm in diameter.
5. Adults produce microfilariae measuring 250 to 300 µm by 6 to 8 μm, which are sheathed and have diurnal periodicity.
6. Microfilariae have been recovered from spinal fluids, urine, and sputum.
7. Loa loa parasites are found in certain rainy forests of C. & W. Africa
LOA LOA TRANSMISSION AND CYCLE
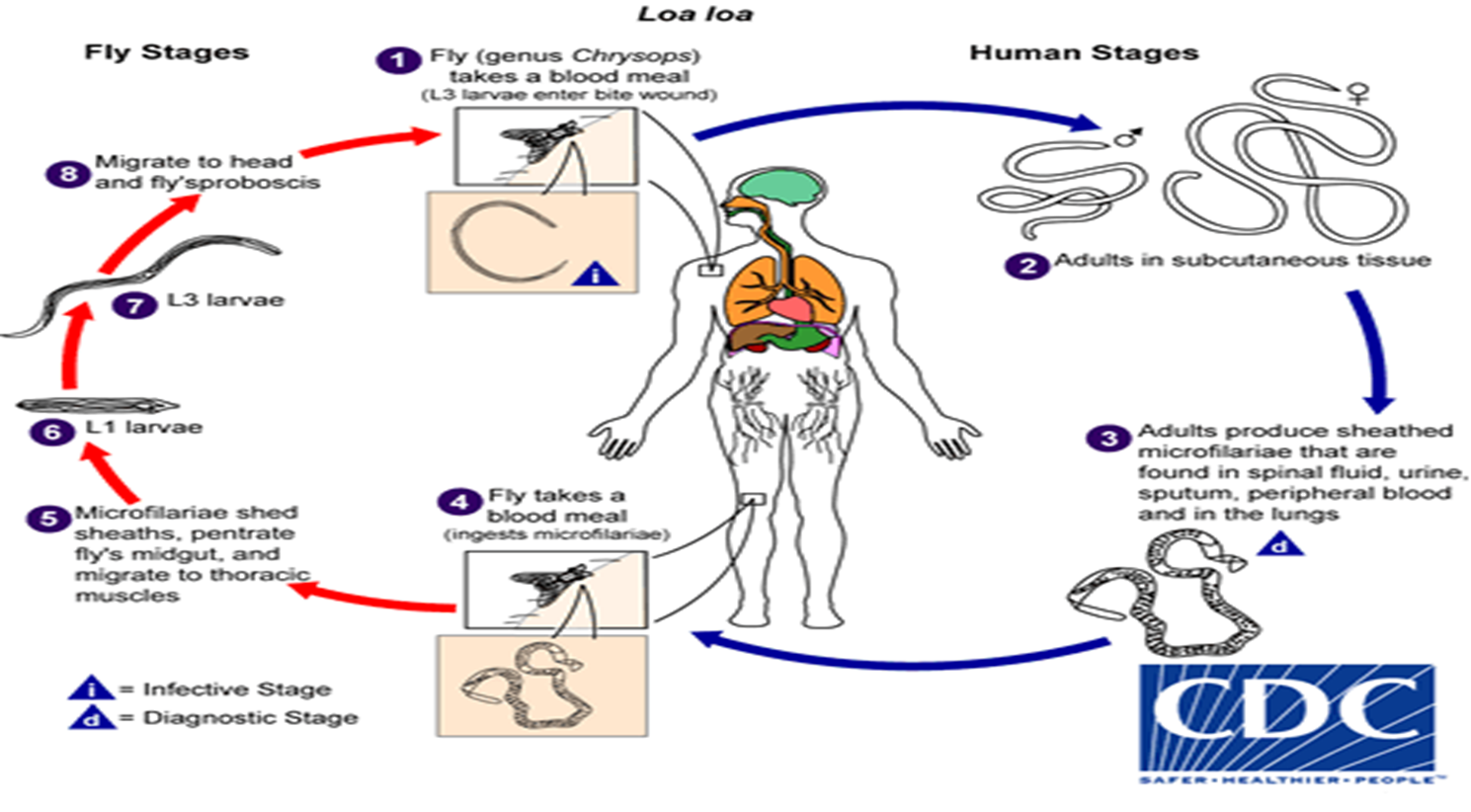
1. During a blood meal, an infected fly (genus Chrysops, day-biting flies) introduces third-stage filarial larvae onto the skin of the human host, where they penetrate into the bite wound.
2. The larvae develop into adults that commonly reside in layers of connective tissue (e.g., ligaments, tendons) under the skin and between the thin layers of tissue that cover muscles (fascia).
3. During the day they are found in peripheral blood, but during the noncirculation phase, they are found in the lungs.
4. The fly ingests microfilariae during a blood meal.
5. The microfilariae lose their sheaths and migrate from the fly’s midgut through the hemocoel to the thoracic muscles of the arthropod.
6. There the microfilariae develop into first-stage larvae
7. and subsequently into third-stage infective larvae.
8. The third-stage infective larvae migrate to the fly’s proboscis, and can infect another human when the fly takes a blood meal
LOA LOA PATHOGENESIS AND CLINICAL PRESENTATION
1. Loiasis is often asymptomatic.
2. Episodic angioedema (Calabar swellings) and subconjunctival migration of an adult worm can occur.
3. In non-immune persons, infection with L. loa can cause severe allergic reactions.
LOA LOA LAB DIAGNOSIS
1. Loa loa is usually diagnosed by the finding of microfilaria in peripheral blood smears or adults in the subconjunctiva.
2. The blood films may be thick or thin and stained with Giemsa or hematoxylin-and-eosin.
3. Microfilariae of L. loa exhibit diurnal periodicity and a diagnosis is best made from blood collected during the mid-day (10 AM-2 PM).
LOA LOATREATMENT
1. Surgical removal of adult worms moving under the skin or across the eye can be done.
2. The treatment of choice is diethylcarbamazine (DEC), which kills the microfilariae and adult worms.
3. Albendazole is sometimes used in patients who are not cured with multiple DEC treatments. It is thought to kill adult worms.
4. Sometimes, other medical conditions need to be addressed first in order to make it safer to use DEC.
LOA LOA LAB PREVENTION AND CONTROL
1. There are no vaccines that protect you from loiasis.
2. If you are going to be in an area with loiasis for a long period of time, diethylcarbamazine (DEC)—300mg taken once a week—can reduce your risk of infection.
3. Avoiding areas where the deerflies are found, such as muddy, shaded areas along rivers or around wood fires.
4. You may reduce your risk of bites by using insect repellants that contain DEET (N,N-Diethyl-meta-toluamide) and wearing long sleeves and long pants during the day.
5. Treating your clothes with permethrin.
Click below for;
PERIODICITY, SPECIMEN COLLECTION DIFFERENTIAL LAB. EXAMINATION OF VARIOUS BLOOD MICROFILARIA
ONCHOCERCA VOLVULUS INTRODUCTION

1. Onchocerca volvulus causes onchocerciasis (river blindness).
2. Additionally, onchocerciasis can cause skin disease, including intense itching, rashes, or nodules under the skin.
Images: Left/Right: Blackflies, the vector of onchocerciasis.
3. Center: Microfilariae of O. volvulus from a skin nodule, stained with H&E. Image taken at 1000x oil magnification. (Credit: WHO, DPDx, CDC)
occurs mainly in Africa, with additional foci in Latin America and the Middle East
4. The microfilariae, measuring 220 to 360 µm by 5 to 9 µm and unsheathed, have a life span that may reach 2 years
5. Adult females measure 33 to 50 cm in length and 270 to 400 µm in diameter, while males measure 19 to 42 mm by 130 to 210 µm.
6. Occurs mainly in Africa, sub-Saharan Africa with additional foci in Latin America and Yemen, the Middle East.
ONCHOCERCA VOLVULUS TRANSMISSION AND LIFE CYCLE
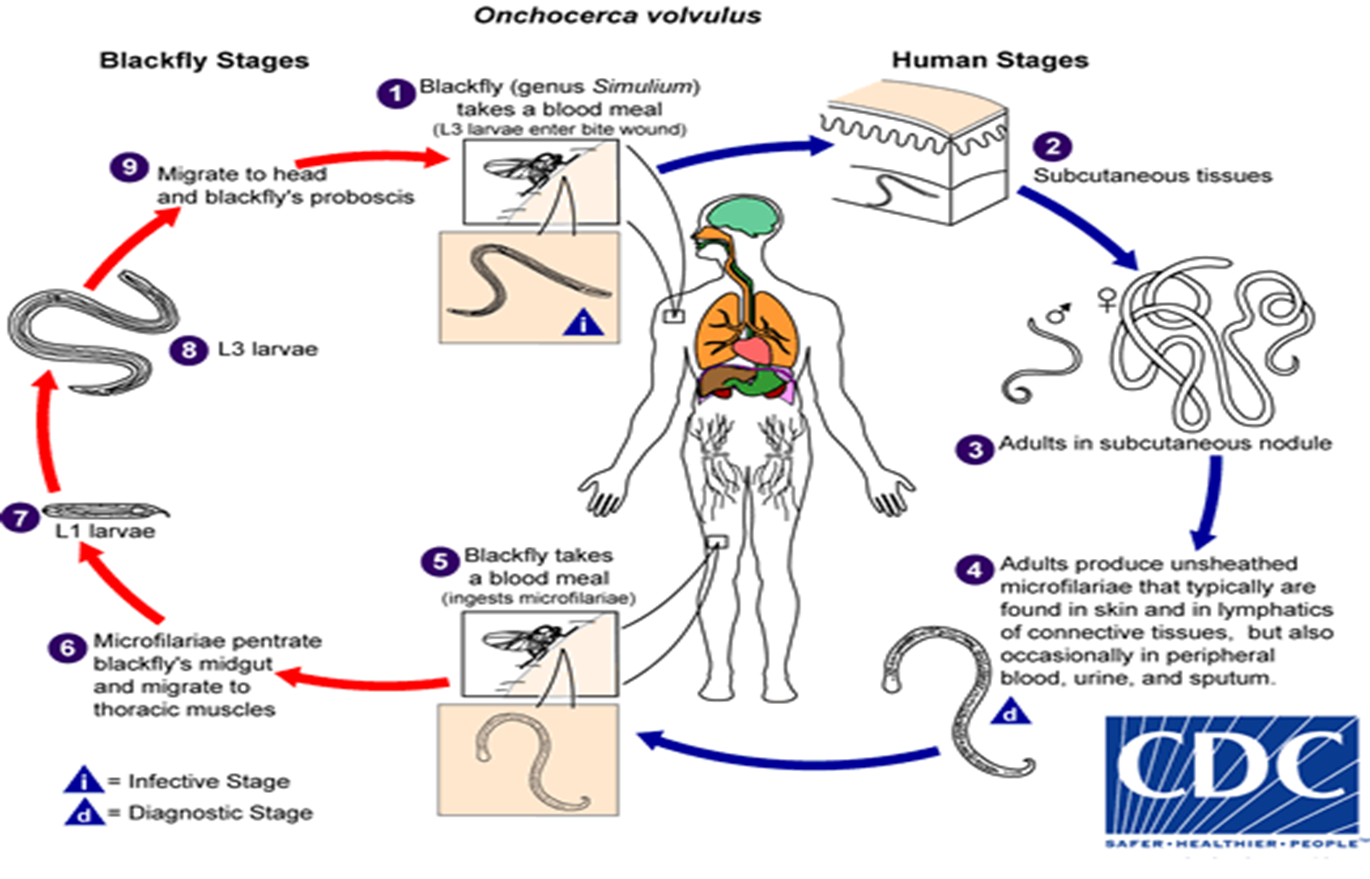
1. During a blood meal, an infected blackfly (genus Simulium) introduces infective filarial larvae onto the skin of the human host, where they penetrate into the bite wound.
2. In subcutaneous tissues the larvae develop into adult filariae,
3. which commonly reside in nodules in subcutaneous connective tissues
4. They are occasionally found in peripheral blood, urine, and sputum but are typically found in the skin and in the lymphatics of connective tissues.
5. A blackfly ingests the microfilariae during a blood meal.
6. The microfilariae migrate from the blackfly’s midgut through the hemocoel to the thoracic muscles.
7. There the microfilariae develop into first-stage larvae and
8. Subsequently into third-stage infective larvae.
9. Which migrate to the blackfly’s proboscisa nd can infect another human when the fly takes a blood meal.
ONCHOCERCA VOLVULUS PATHOGENESIS AND CLINICAL PRESENTATION
1. Onchocerciasis can cause pruritus, dermatitis, onchocercomata (subcutaneous nodules), and lymphadenopathies.
2. The most serious manifestation consists of ocular lesions that can progress to blindness.
ONCHOCERCA VOLVULUS LAB DIAGNOSIS
1. The most common method of diagnosis is the skin snip. A 1 to 2 mg shaving or biopsy of the skin is done to identify larvae, which emerge from the skin snip and can be seen under a microscope when the shaving or biopsy (“skin snip”) is put in physiologic solutions (e.g. normal saline). Typically six snips are taken from different areas of the body.
2. In patients with nodules in the skin, the nodule can be surgically removed and examined for adult worms.
3. Infections in the eye can be diagnosed with a slit-lamp examination of the anterior part of the eye where the larvae, or the lesions they cause, are visible.
4. Polymerase chain reaction (PCR) of the skin snip can allow for diagnosis if the larvae are not visualized.
5. Antibody tests have been developed to test for infection, they are useful in visitors to these endemic areas, they are not as useful in people who lived in areas where the parasite exists.
6. Some of the tests are general tests for infection with any filarial parasite and some are more specific for onchocerciasis.
ONCHOCERCA VOLVULUS TREATMENT
1. The recommended treatment is ivermectin, it kills the larvae and prevents them from causing damage but it does not kill the adults.
2. Doxycycline that kills the adult worms by killing the Wolbachia bacteria on which the adult worms depend in order to survive.
3. Treament with both ivermectin and doxycycline is likely.
4. Loa loa can be responsible for severe side effects to the medications used to treat onchocerciasis.
ONCHOCERCA VOLVULUS PREVENTION AND CONTROL
1. There are no vaccines or medications available to prevent becoming infected with O. volvulus.
2. The best prevention efforts include wearing insect repellant such as N,N-Diethyl-meta-toluamide (DEET) on exposed skin, wearing long sleeves and long pants during the day when blackflies bite, and wearing permethrin- treated clothing.
3. Mass distribution of ivermectin to all people living in many areas where O. volvulus is found, is being given to control onchocerciasis.
DRACUNCULUS MEDINENSIS INTRODUCTION

1. Dracunculiasis (Guinea worm disease) is caused by the nematode (roundworm) Dracunculus medinensis.
2. Image;
Left: The female Guinea worm induces a painful blister.
Right: Using a matchstick to wind up and remove a guinea worm from the leg of a human.
3 The females (length: 70 to 120 cm).
4 GWD affects poor communities in remote parts of Africa that do not have safe water to drink. Chad is an example
DRACUNCULUS MEDINENSIS TRANSMISSION AND LIFE CYCLE
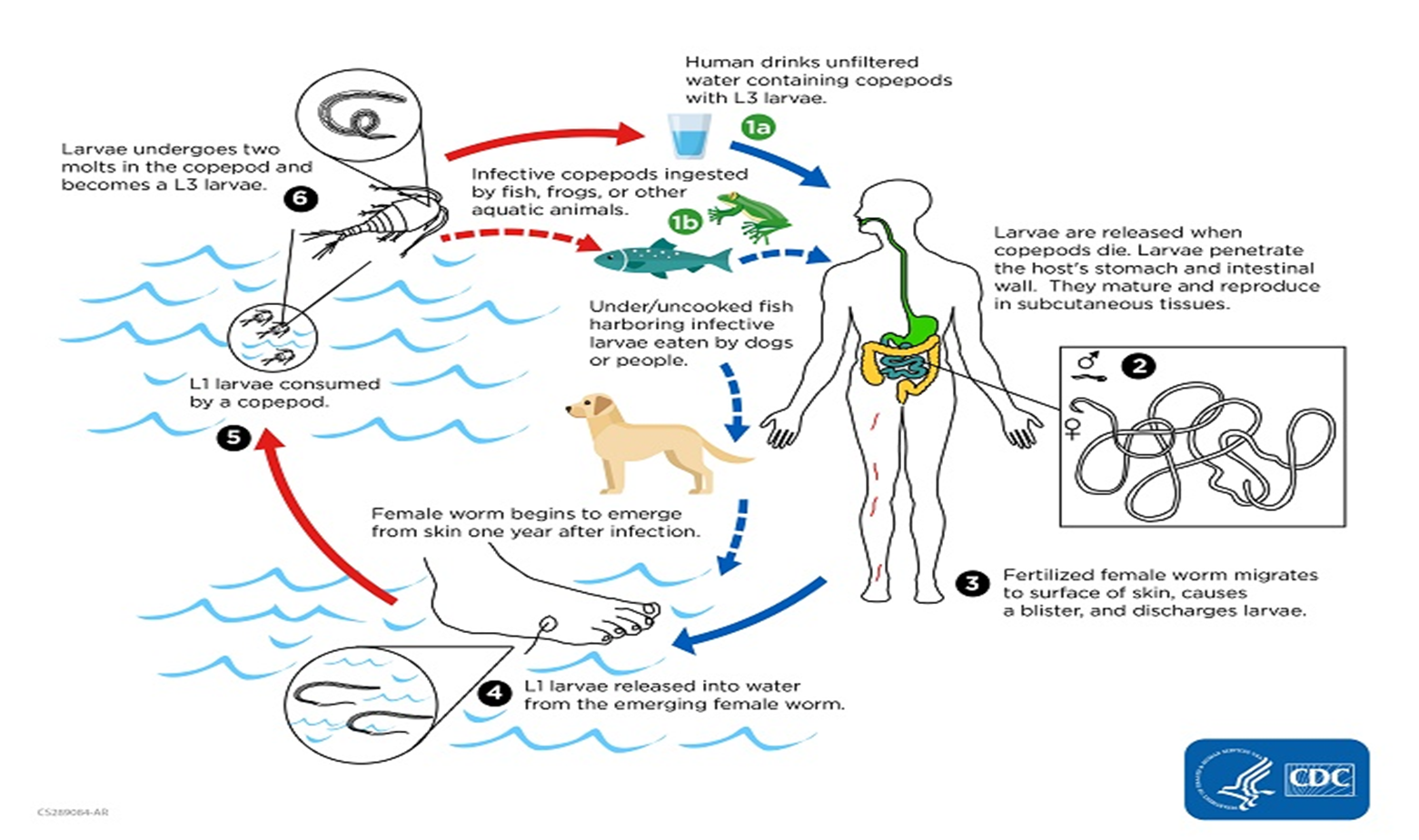
1 Humans become infected by drinking unfiltered water containing copepods (small crustaceans) which are infected with larvae of D. medinensis.
2 The copepods die and release the larvae, which penetrate the host stomach and intestinal wall and enter the abdominal cavity and retroperitoneal space.
3 After maturation into adults and copulation, the male worms die and the females migrate in the subcutaneous tissues towards the skin surface.
4 Approximately one year after infection, the female worm induces a blister on the skin, generally on the distal lower extremity, which ruptures. When this lesion comes into contact with water, a contact that the patient seeks to relieve the local discomfort, the female worm emerges and releases larvae.
5 The larvae are ingested by a copepod and
6 after two weeks (and two molts) have developed into infective larvae and the cycle repeats.
DRACUNCULUS MEDINENSIS CLINICAL MANIFESTATIONS
1 The clinical manifestations are localized but incapacitating.
2 The worm emerges as a whitish filament (duration of emergence: 1 to 3 weeks) in the center of a painful ulcer.
3 Accompanied by inflammation and frequently by secondary bacterial infection.
DRACUNCULUS MEDINENSIS TREATMENT MANAGEMENT
1. There is no specific drug to treat or prevent GWD. There is also no vaccine to prevent GWD.
Optimal management of GWD involves the following steps:
2. First, the infected person is not allowed to enter drinking water sources.
3. Next, the wound is cleaned. The affected body part may be immersed or soaked in water (far away from any water source to prevent contamination) to encourage the worm to contract and release larvae. Emptying the worm of larvae may make removing the worm easier.
4. The worm is then wrapped around a rolled piece of gauze or a stick to maintain some tension on the worm and encourage more of the worm to emerge. This also prevents the worm from slipping back inside.
5. Pulling gently stops when resistance is met to avoid breaking the worm, full extraction can take several days to weeks.
6. The affected body part is then bandaged with fresh gauze to protect the site. Medicines, such as aspirin or ibuprofen and antibiotics, are given to help ease the pain of this process and reduce inflammation and secondary infections.
DRACUNCULUS MEDINENSIS PREVENTION AND CONTROL
Prevention of GWD is based on the following:
1. Surveillance (case detection) and case containment (preventing contamination of drinking water sources by infected persons or animals)
2. Provision of safe drinking water
3. Vector control (killing of the copepods involved in the Guinea worm life cycle) using the approved chemical temephos
4. Health education and community mobilization
ECHINOCOCCUS SPECIES INTRODUCTION
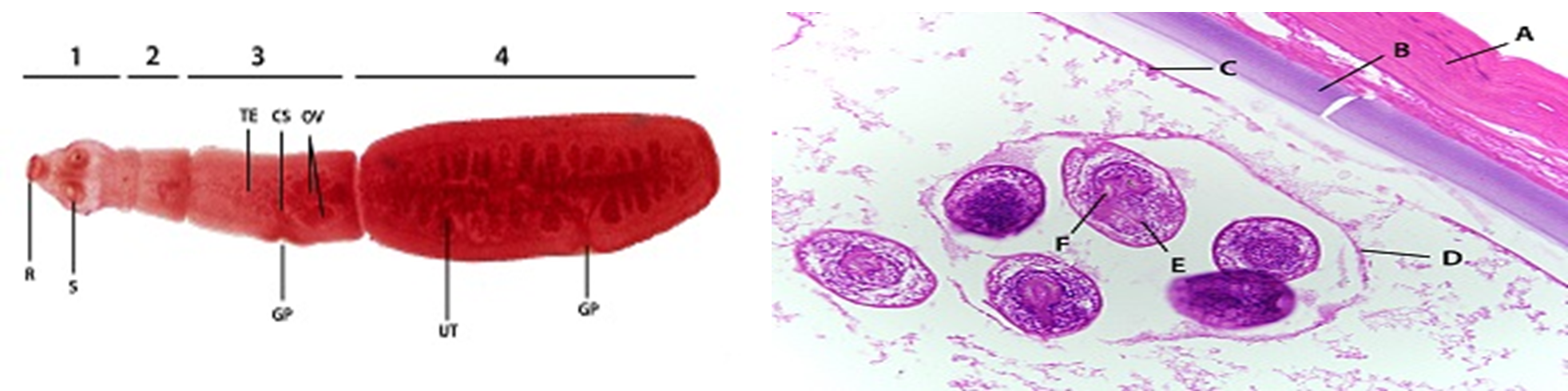
1. Left: Echinococcus granulosus adult (2—7 mm long), stained with carmine. This spicies has four segments (1: scolex; 2: immature proglottid; 3: mature proglottid; 4: gravid proglottid). Features highlighted are the armed rostellum (R) and suckers (S) of the scolex, and reproductive structures including the testes (TE), cirrus sac (CS), ovaries (OV), branched uterus containing eggs (UT), and genital pores on the mature and gravid proglottids (GP).
2. Right: Cross-section of an E. granulosus cyst, stained with H&E. Host tissue (A) encapsulates the hydatid cyst wall, which is composed of an acellular laminated layer (B) and a nucleate germinal layer (C) from which the brood capsule (D) arises. Inside the brood capsule are numerous protoscolices (E) with visible hooklets (F).
3. These cysts can be found in any part of the body, but are most common in the liver, lung and central nervous system causing Echinococcosis
4. Human echinococcosis (hydatidosis, or hydatid disease) is caused by the larval stages of cestodes (tapeworms) of the genus Echinococcus
5. Echinococcus granulosus (sensu lato) causes cystic echinococcosis and is the form most frequently encountered.
6. Another species, E. multilocularis, causes alveolar echinococcosis, and is becoming increasingly more common.
7. Two exclusively New World species, E. vogeli and E. oligarthrus, are associated with “Neotropical echinococcosis”; E. vogeli causes a polycystic form whereas E. oligarthrus causes the extremely rare unicystic form.
8. E. granulosus is found in Africa, Europe, Asia, the Middle East, Central and South America, and in rare cases, North America. Causes Cystic echinococcosis (CE).
9. Echinococcus multilocularis is found across the globe and is especially prevalent in the northern latitudes of Europe, Asia, and North America. Causes Alveolar echinococcosis (AE).
ECHINOCOCCUS SPECIES TRANSMISSION AND LIE CYCLE
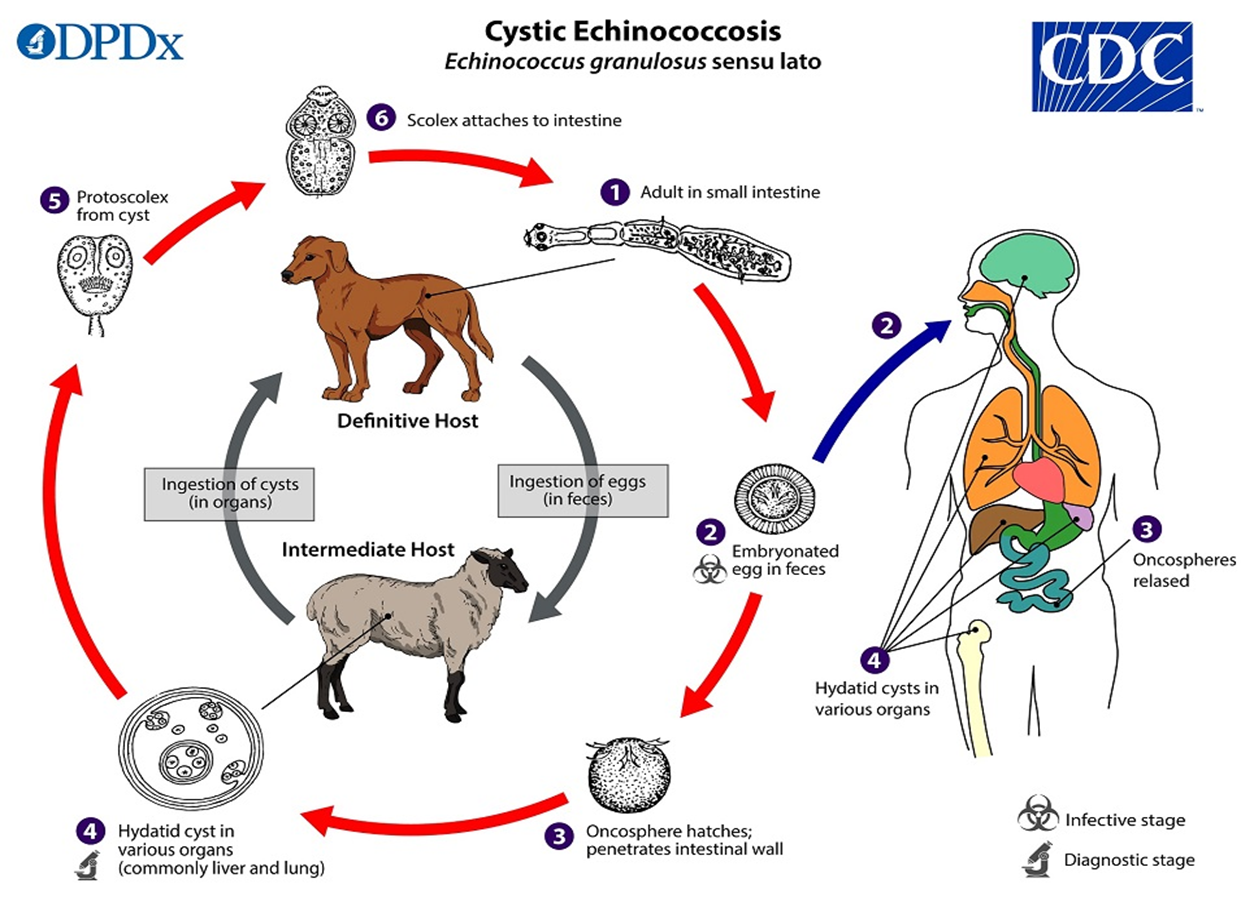
1. The adult Echinococcus granulosus resides in the small intestine of the definitive host.
2. Gravid proglottids release eggs image that are passed in the feces, and are immediately infectious.
3. After ingestion by a suitable intermediate host, eggs hatch in the small intestine and release six-hooked oncospheres that penetrate the intestinal wall and migrate through the circulatory system into various organs, especially the liver and lungs.
4. In these organs, the oncosphere develops into a thick-walled hydatid cyst that enlarges gradually, producing protoscolices and daughter cysts that fill the cyst interior.
5. The definitive host becomes infected by ingesting the cyst-containing organs of the infected intermediate host.
6. After ingestion, the protoscolices evaginate, attach to the intestinal mucosa image, and develop into adult stages in 32 to 80 days and the cycle repeats.
7. Humans are aberrant intermediate hosts, and become infected by ingesting eggs.
8. Oncospheres are released in the intestine, and
9. hydatid cysts develop in a variety of organs.
10. If cysts rupture, the liberated protoscolices may create secondary cysts in other sites within the body (secondary echinococcosis).
11. Other Echinococcus spp follow a similar life cycle with changes in the definitive and intermediate hosts and the range of human organs attacked.
ECHINOCOCCUS SPECIES PATHOGENESIS AND CLINICAL PRESENTATION
1. Echinococcus granulosus: In addition to the liver and lungs, the most common sites affected, other organs (spleen, kidneys, heart, bone, and central nervous system, including the brain and eyes) can also be involved, with resulting symptoms. Rupture of the cysts can produce a host reaction manifesting as fever, urticaria, eosinophilia, and potentially anaphylactic shock; rupture of the cyst may also lead to cyst dissemination.
2. Echinococcus multilocularis affects the liver as a slow growing, destructive tumor, often with abdominal pain and biliary obstruction being the only manifestations evident in early infection. This may be misdiagnosed as liver cancer. Rarely, metastatic lesions into the lungs, spleen, and brain occur. Untreated infections have a high fatality rate.
3. Echinococcus vogeli affects mainly the liver, where it acts as a slow growing tumor; secondary cystic development is common. Too few cases of E. oligarthrus have been reported for characterization of its clinical presentation.
ECHINOCOCCUS SPECIES LAB. DIAGNOSIS
1. Imaging techniques, such as CT scans, ultrasonography, and MRIs, are used to detect cysts.
2. After a cyst has been detected, serologic tests may be used to confirm the diagnosis.
3. In seronegative patients with hepatic image findings compatible with echinococcosis, ultrasound guided fine needle biopsy may be useful for confirmation of diagnosis.
4. False-positive reactions may occur in persons with other cestode infections, some other helminth infections, cancer, and liver cirrhosis
ECHINOCOCCUS SPECIES TREATMENT
1. The treatment of alveolar echinococcosis is more difficult than cystic echinococcosis and usually requires radical surgery, long-term chemotherapy, or both.
2. Chemotherapy, cyst puncture, and PAIR (percutaneous aspiration, injection of chemicals and reaspiration) have been used to replace surgery as effective treatments for cystic echinococcosis.
3. However, surgery remains the most effective treatment to remove the cyst and can lead to a complete cure.
ECHINOCOCCUS SPECIES PREVENTION AND CONTROL
Cystic Echinococcosis
1. Prevent dogs from feeding on the carcasses of infected sheep.
2. Control stray dog populations.
3. Restrict home slaughter of sheep and other livestock.
4. Do not consume any food or water that may have been contaminated by fecal matter from dogs.
5. Wash your hands with soap and warm water after handling dogs, and before handling food.
6. Teach children the importance of washing hands to prevent infection.
Alveolar Echinococcosis
1. Do not allow dogs to feed on rodents and other wild animals.
2. Avoid contact with wild animals such as foxes, coyotes and stray dogs.
3. Do not encourage wild animals to come close to your home or keep them as pets.
4. Wash your hands with soap and warm water after handling dogs or cats, and before handling food.
5. Teach children the importance of washing hands to prevent infection.
TRICHINELLA SPECIES INTRODUCTION
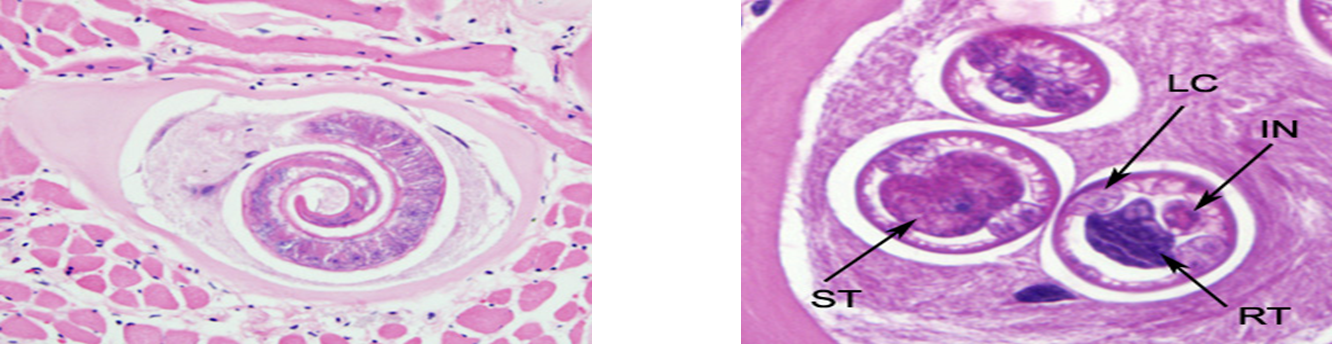
1. Left: richinella larva in tongue muscle of a rat, stained with hematoxylin and eosin (H&E). Image was captured at 400x magnification.
2. Right: Shown in these cuts are a nucleated stichocyte (ST), prominent lateral chords, or bacillary bands, (LC), immature reproductive tubes (RT), and the intestine (IN). Image captured at 1000x magnification.
3. Nematodes (roundworms) of the genus Trichinella cause Trichinellosis (trichinosis) disease.
4. Females are 2.2 mm in length; males 1.2 mm.
5. The classical agent T. spiralis found worldwide. Most common in parts of Europe and the United States, (in many carnivorous and omnivorous animals).
6. Several other species including T. pseudospiralis (mammals and birds worldwide),
7. T. nativa (Arctic bears), T. nelsoni (African predators and scavengers),
8. T. britovi (carnivores of Europe and western Asia), and
9. T. papuae (wild and domestic pigs, Papua New Guinea and Thailand).
10. Trichinella zimbabwensis is found in crocodiles in Africa but to date there are no known associations of this species with human disease.
TRICHINELLA SPECIES TRANSMISSION AND LIFE CYCLE
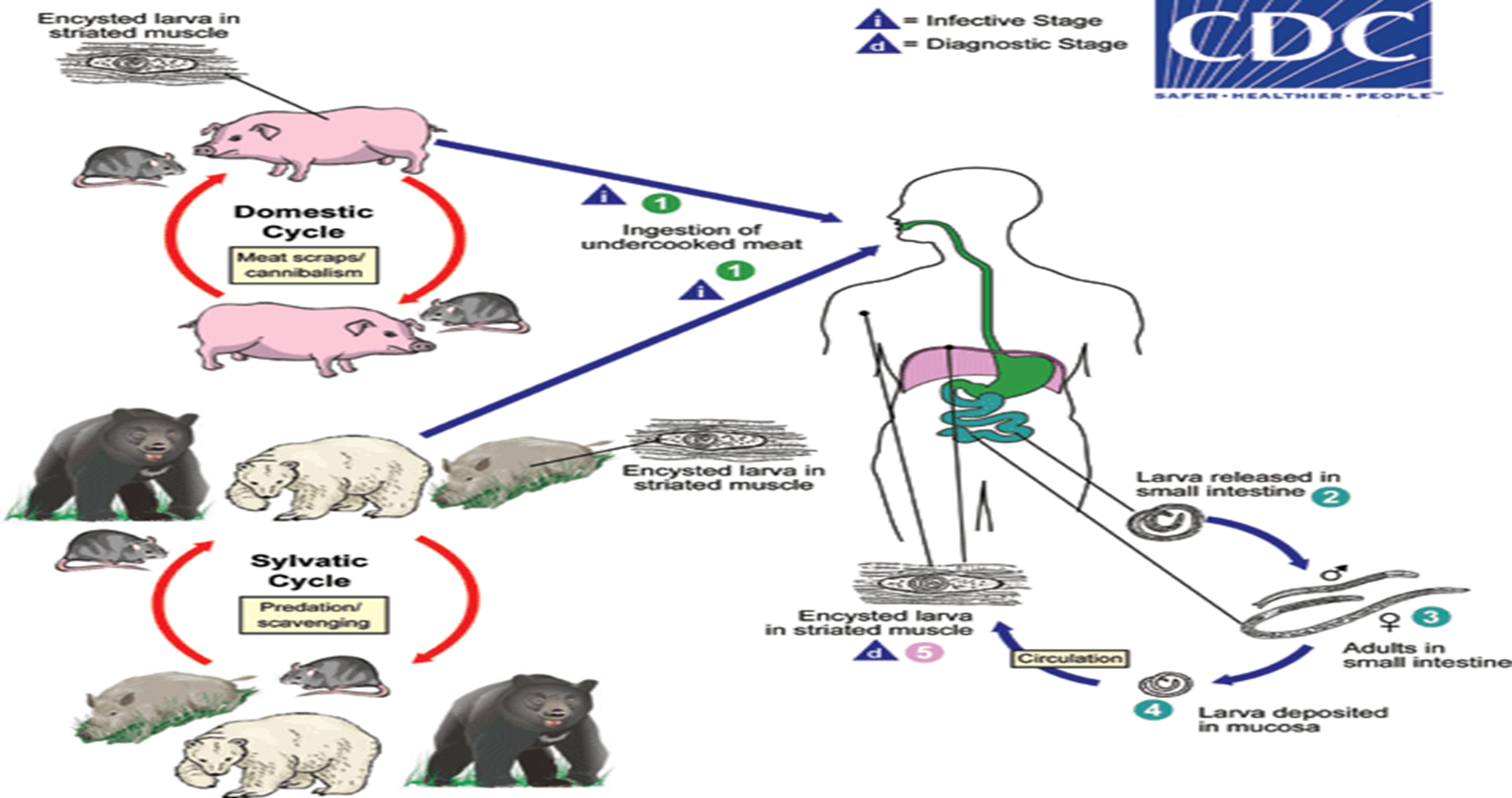
1. Trichinellosis is caused by the ingestion of undercooked meat containing encysted larvae (except for T. pseudospiralis and T. papuae, which do not encyst) of Trichinella species.
2. After exposure to gastric acid and pepsin, the larvae are released from the cysts and
3. Invade the small bowel mucosa where they develop into adult worms.
4. After 1 week, the females release larvae that
5. Migrate to striated muscles where they encyst.
TRICHINELLA SPECIES CLINICAL PRESENTATION
1. Light infections may be asymptomatic.
2. Intestinal invasion can be accompanied by gastrointestinal symptoms (diarrhea, abdominal pain, vomiting).
3. Larval migration into muscle tissues (one week after infection) can cause periorbital and facial edema, conjunctivitis, fever, myalgias, splinter hemorrhages, rashes, and peripheral eosinophilia.
4. Occasional life-threatening manifestations include myocarditis, central nervous system involvement, and pneumonitis.
5. Larval encystment in the muscles causes myalgia and weakness, followed by subsidence of symptoms.
TRICHINELLA SPECIES LAB. DIAGNOSIS
Diagnosis is usually made based on clinical symptoms, and is confirmed by serology or identification of encysted or non-encysted larvae in biopsy or autopsy specimens.
TRICHINELLA SPECIES TREATMENT
Treatment with either mebendazole or albendazole is recommended
TRICHINELLA SPECIES PREVENTION AND CONTROL
1. The best way to prevent trichinellosis is to cook meat to safe temperatures until its ready.
2. Wash your hands with warm water and soap after handling raw meat.
3. Curing (salting), drying, smoking, or microwaving meat alone does not consistently kill infective worms.
4. Freeze pork less than 6 inches thick for 20 days at 5°F (-15°C) to kill any worms.
5. Unlike freezing pork products, some worm species that infect wild game animals are freeze-resistant.
6. Clean meat grinders thoroughly after each use.
TOXOCARA SPECIES INTRODUCTION
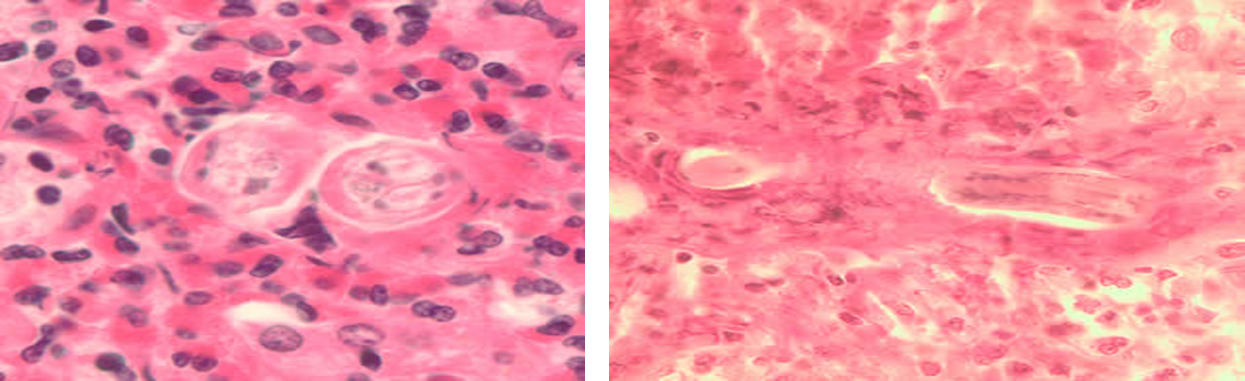
1. Left: Cross-section of Toxocara sp. larvae in liver tissue stained with hematoxylin and eosin (H&E).
2. Right: Longitudinal section of a Toxocara sp. larva in lung tissue stained with H&E.
3. Toxocara spp., are common ascarid roundworms of mammals.
4. Confirmed zoonotic species include the dog roundworm T. canis (presumed most common) and the cat roundworm T. cati (frequency not known).
5. It is not known whether other closely-related Toxocara species can infect humans (e.g. T. malaysiensis of cats).
6. There are two major forms of toxocariasis, visceral toxocariasis (VT), also called visceral larva migrans (VLM), and ocular toxocariasis (OT), also called ocular larva migrans (OLM).
7. Globally, toxocariasis is found in many countries, and prevalence rates can reach as high as 40% or more in parts of the world.
8. While common globally, prevalence in both animals and people is highest in developing countries.
9. Toxocara is more prevalent in hot, humid regions where eggs are able to survive better in the soil.
10. People are more likely to be infected with Toxocara if they own a dog.
11. Cockroaches and earthworms have been experimentally infected, and could possibly serve as paratenic or transport hosts.
TOXOCARA SPECIES TRANSMISSION AND LIFE CYCLE
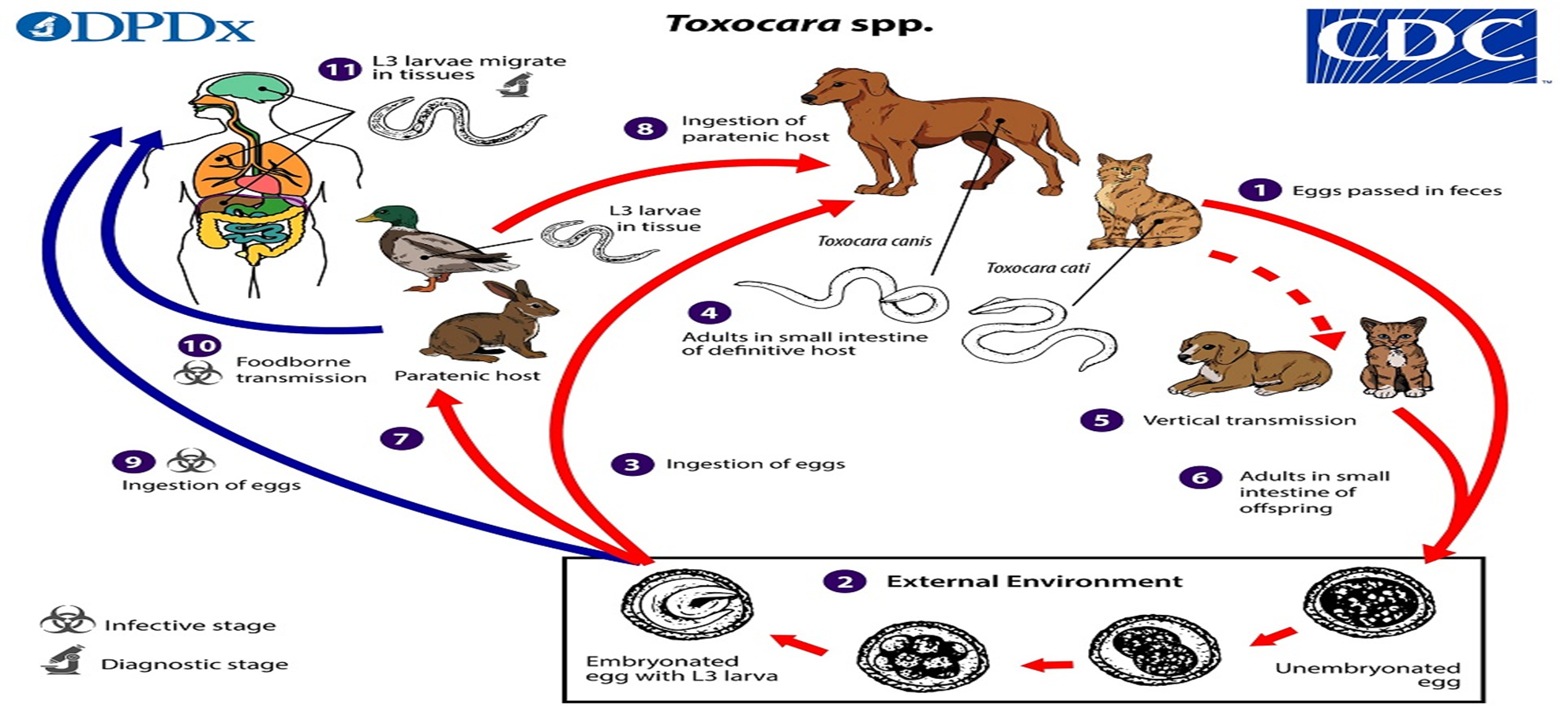
Toxocara spp. can follow a direct (one host) or indirect (multiple host) life cycle.
1. Unembryonated eggs are shed in the feces of the definitive host (canids: T. canis; felids: T. cati).
2. Eggs embryonate over a period of 1 to 4 weeks in the environment and become L3 infective larvae.
3. Following ingestion by a definitive host,
4. the infective eggs hatch and larvae penetrate the gut wall. In younger dogs (T. canis) and in cats (T. cati), the larvae migrate through the lungs, bronchial tree, and esophagus, where they are coughed up swallowed into the gastrointestinal tract; adult worms develop and oviposit in the small intestine.
5. In older dogs, patent (egg-producing) infections can also occur, but larvae more commonly become arrested in tissues. Arrested larvae are reactivated in female dogs during late gestation and may infect pups by the transplacental (major) and transmammary (minor) route in whose small intestine adult worms become established.
6. In cats, T. cati larvae can be transmitted via the transmammary route image to kittens if the dam is infected during gestation, but somatic larval arrest and reactivation does not appear to be important as in T. canis.
Toxocara spp. can also be transmitted indirectly through ingestion of paratenic hosts.
7. Eggs ingested by suitable paratenic hosts hatch and larvae penetrate the gut wall and migrate into various tissues where they encyst. The life cycle is completed when definitive hosts consume larvae within paratenic host tissue, and
8. the larvae develop into adult worms in the small intestine.
9. Humans are accidental hosts who become infected by ingesting infective eggs or undercooked meat/viscera of infected paratenic hosts.
10. After ingestion, the eggs hatch and larvae penetrate the intestinal wall and are carried by the circulation to a variety of tissues (liver, heart, lungs, brain, muscle, eyes).
While the larvae do not undergo any further development in these sites, they can cause local reactions and mechanical damage that causes clinical toxocariasis.
TOXOCARA SPECIES CLINICAL PRESENTATION
The most visceral larva migrans (VLM) and ocular larva migrans (OLM), infections are asymptomatic, however;
1. Can cause various nonspecific symptoms (e.g. fever, myalgia, weight loss, cough, rashes, hepatosplenomegaly).
2. Usually accompanied by hypereosinophilia.
3. Neurotoxocariasis or neural larva migrans (NLM)) though, uncommon can cause eosinophilic meningoencephalitis.
4. In OLM, with associated visual impairment usually presents with uveitis, retinitis, or endophthalmitis; permanent visual damage or blindness can occur. Associated larval granulomas have in some cases have been misdiagnosed as retinoblastoma.
TOXOCARA SPECIES LAB DIAGNOSIS
Diagnosis is usually made based on clinical symptoms, and is confirmed by
1. Serology or
2. Identification of encysted or non-encysted larvae in biopsy or autopsy specimens.
TOXOCARA SPECIES PREVENTION AND CONTROL
1. Regular treating of the worm infection in dogs and cats will control risk of infection for people.
2. Clean your pet’s living area at least once a week; every day is better.
3. Do not allow children to play in areas that are soiled with pet or other animal feces and cover sandboxes when not in use.
4. Prompt removal of animal feces since the eggs require 2 to 4 weeks to become infective.
5. Although rare, people can also be infected by eating undercooked or raw meat from an infected animal such as a lamb or rabbit.
ZOONOTIC HOOKWORM INTRODUCTION

Image:
Left: Discrete, non-bullous CLM on ankle.
Center: Erythematous and bullous CLM on ankle.
Right: Filariform (L3) hookworm larvae which are found in the environment and infect the human host by penetration of the skin.
Zoonotic hookworms are hookworms that live in animals but can be transmitted to humans.
1. Dogs and cats can become infected with several hookworm species, including Ancylostoma brazilense, A. caninum, A. ceylanicum, and Uncinaria stenocephala.
2. Bunostomum phlebotomum, a cattle hookworm, is also capable of causing short-lived CLM in humans.
3. Worldwide, especially tropical and subtropical regions, including: southeastern United States, Latin America, S. America, Australasian and Africa where we find A. braziliense. Uncinaria stenocephala is found Americas, Europe, Asia, Australia, and New Zealand.
ZOONOTIC HOOKWORM TRANSMISSION AND LIFE CYCLE
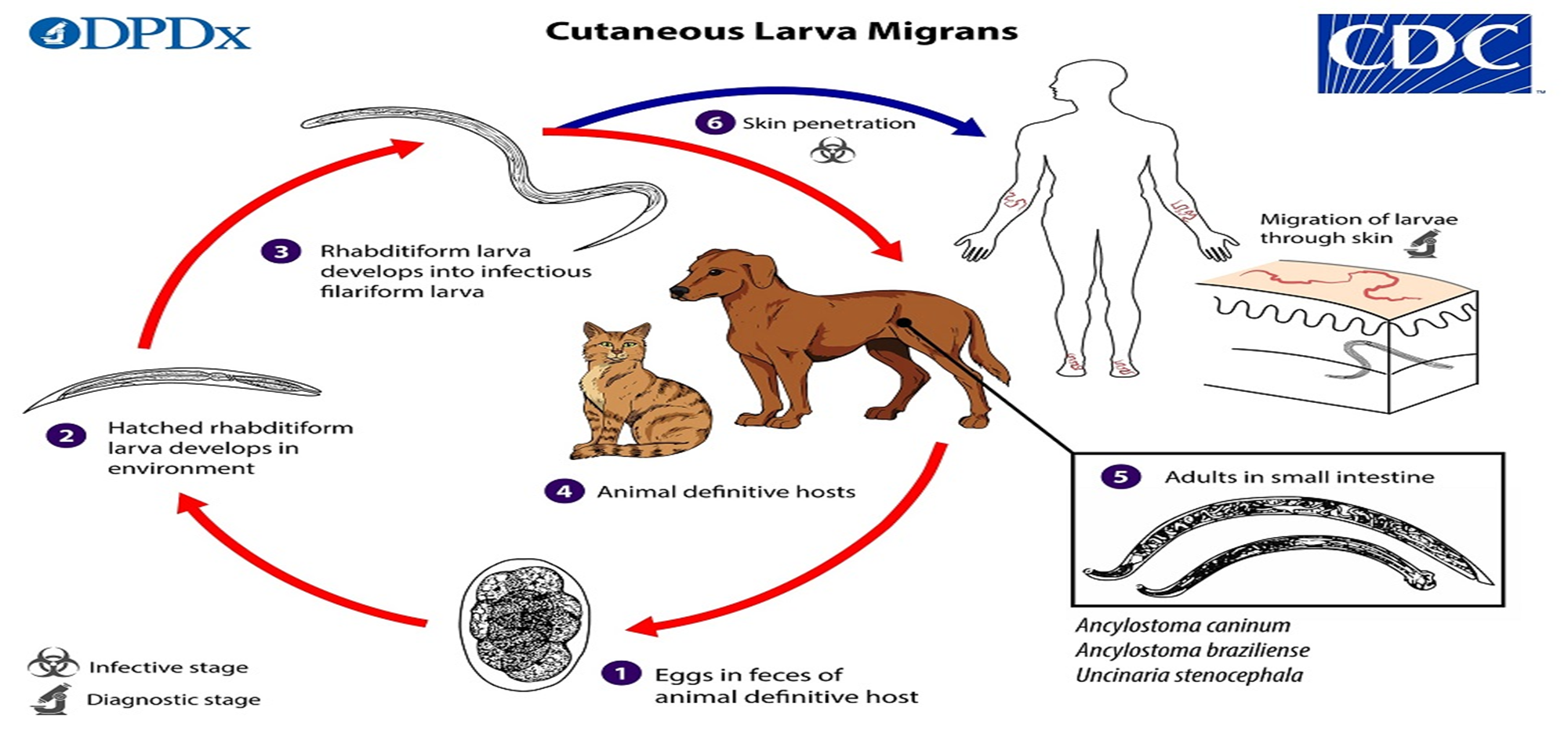
1. Eggs are passed in the animal definitive host’s stool,
2. Larvae hatch in 1 to 2 days and the released rhabditiform larvae grow in the feces and/or the soil, and
3. After 5 to 10 days (and 2 molts) they become filariform (third-stage) larvae that are infective.
4. These infective larvae can survive 3 to 4 weeks and on contact with the animal host,
5. the larvae penetrate the skin and are carried through the blood vessels to the heart and then to the lungs, ascend the bronchial tree to the pharynx, and are swallowed.
6. The larvae reach the small intestine, where they reside and mature into adults. Some larvae become arrested in the tissues, and serve as source of infection for pups via transmammary (and possibly trans placental) routes.
7. Humans become infected when filariform larvae penetrate the skin.
With most species, the larvae cannot mature further in the human host and migrate aimlessly within the epidermis, sometimes as much as several centimeters a day. Some larvae may become arrested in deeper tissue after skin migration.
ZOONOTIC HOOKWORM CLINICAL PRESENTATION
1. The most common manifestation of zoonotic infection with animal hookworm species is cutaneous larva migrans (CLM).
2. CLM is also known as creeping eruption, where migrating larvae cause intensely pruritic and erythematous serpiginous tracks in the upper dermis, which may occasionally become bullous.
3. These tracks may spread up to a few centimeters daily, and secondary infections can develop following excessive scratching.
4. In some cases of diffuse unilateral subacute retinitis, single larvae compatible in size with Ancylostoma spp. have been visualized in the affected eye.
ZOONOTIC HOOKWORM LAB. DIAGNOSIS
1. Cutaneous larva migrans is diagnosed clinically, as there are no serologic tests for zoonotic hookworm infections.
2. Larvae may be seen in stained tissue sections, but this procedure is not recommended as the parasites are usually not found in the visible track.
3. Usually, extensive eosinophilic infiltration is seen in skin biopsies.
ZOONOTIC HOOKWORM TREATMENT
1. Treatment with albendazole or ivermectin are curative.
2. Children younger than 2 years of age or under 15 kg body weight may be treated with topical preparations.
ZOONOTIC HOOKWORM PREVENTION AND CONTROL
1. Regular veterinary care for your pets - including deworming - will help ensure healthy pets and healthy people.
2. Prompt disposal of animal feces before eggs hatching and contaminating soil.
3. Wearing shoes and use protective mats or other coverings to prevent direct skin contact with sand or soil.
Last modified: Saturday, 18 April 2026, 11:04 PM
Background Colour
Font Face
Font Kerning
Font Size
1
Image Visibility
Letter Spacing
0
Line Height
1.2
Link Highlight
Text Alignment
Text Colour