
Completion requirements
Course Outline
1. Introduction
2. Terms and definitions related to parasitology
3. Host-parasites relationship/interactions
4. Basic and principal concepts in medical parasitology
5. Classification of medically important parasites
6. General characteristics for parasites
7. Basic diagnostic techniques in the medical parasitology laboratory
INTRODUCTION
Medical parasitology is the science that deals with organisms living in the human body (the host) and the medical significance of this host-parasite relationship and means of fight to them that one can propose.
A parasite is a living organism, which takes its nourishment and other needs from a host; the host is an organism which supports the parasite.
The parasites included in medical parasitology are protozoa, helminths, and some arthropods.
The hosts vary depending on whether they harbor the various stages in parasitic development.Medical parasitology aims at triple goals based on several disciplines:
The Biological goal: i.e. knowledge specifies morphology of the parasite itself, consequences of its presence in the human body.
The clinical goal: i.e. the semiology of the diseases determined by the parasites, their diagnosis and their curative treatment.
The Preventive and/or prophylactic goal: i.e. the protection of the healthy man against the parasitoses. Epidemiology.
Epidemiology must preliminary specify the determining conditions and the supporting factors of the infestation.
Infestation: It is the invasion of a living organism or the environment by parasites. It implies determining conditions and others supporting factors
a) Determining conditions
Initially it is the parasite itself with its morphology and its physiology
The intermediate hosts which can be essential to ensure the perfect development of the parasite.
The vectors which ensure the penetration of the parasite at the man
The animals which can lodge parasite and disseminate it (propagate) thus playing the role "of reservoir of parasite"
b) Factors supporting the infestation
They can be of a general nature or individual
Factors of a general nature:
Geographical Factors
Climatic factors
Anthropological Factors:
Mode of live
Culinary practice
Quality and quantity of the food
Religious practice
C. Factors of an individual nature :
The receptivity of the individual healthy, his resistance to the infestation and the evolution even of the disease can be dependent:
With the sex, age, profession of the individual, undercurrent diseases, constitution even of the subject.
Paper for Discussion: Cox F.E.G. History of human parasitology (2002)
TERMS DEFINITIONS RELATED TO PARASITES
Ectoparasite – a parasitic organism that lives on the outer surface of its host, e.g. lice, ticks, mites etc.
Endoparasites – parasites that live inside the body of their host, e.g. Entamoeba histolytica.
Obligate Parasite - This parasite is completely dependent on the host during a segment or all of its life cycle, e.g. Plasmodium spp.
Facultative parasite – an organism that exhibits both parasitic and non-parasitic modes of living and hence does not absolutely depend on the parasitic way of life, but is capable of adapting to it if placed on a host. E.g. Naegleria fowleri
Accidental parasite – when a parasite attacks an unnatural host and survives. E.g. Hymenolepis diminuta (rat tapeworm).
Erratic parasite - is one that wanders in to an organ in which it is not usually found E.g. Entamoeba histolytica in the liver or lung of humans.
TERMS DEFINITIONS RELATED TO HOSTS
Definitive host – a host that harbors a parasiteod of reproduction. in the adult stage or where the parasite undergoes a sexual meth
Intermediate host - harbors the larval stages of the parasite or an asexual cycle of development takes place. In some cases, larval development is completed in two different intermediate hosts, referred to as first and second intermediate hosts.
Paratenic host – a host that serves as a temporary refuge and vehicle for reaching an obligatory host, usually the definitive host, i.e. it is not necessary for the completion of the parasites life cycle.
Reservoir host – a host that makes the parasite available for the transmission to another host and is usually not affected by the infection.
Natural host – a host that is naturally infected with certain species of parasite.
Accidental host – a host that is under normal circumstances not infected with the parasite.
OTHER IMPORTANT DEFINITONS
1. A vector usually insects or other arthropods (mosquito, tsetse fly, tick, flea, lice, etc.) is an agent, usually an insect, that transmits an infection from one human host to another.
Mechanical vector is used to describe a vector which assists in the transfer of parasitic forms between hosts but is not essential in the life cycle of a parasite, e.g. a fly that transfers amoebic cysts from infected faeces to food that is eaten by humans.
Biological vector – ex. the protozoan parasite that causes malaria goes through a stage in its life cycle in the mosquito. Could bacteria use biological vectors?
2. Zoonosis is used to describe an animal infection that is naturally transmissible to humans either directly or indirectly via a vector
HOST-PARASITE INTERACTIONS/RELATIONSHIP
Adaptations to Parasitism
Profound morphological adaptation to their way of life
Specialized attachment organs in the form of suckers and hooks have been developed
Organs not necessary to a parasitic existence are frequently lost or degenerated
Reproductive system is very highly developed in association with increased reproductive capacity
Physiological and biochemical adaptations
Immune evasion
SYMBIOSIS: Any organism that spends a portion or all of its life cycle intimately associated with another organism of a different species is considered as Symbiont (symbiote) and this relationship is called symbiosis (symbiotic relationships). The following are the three common symbiotic relationships between two organisms:
Mutualism - an association in which both partners are metabolically dependent upon each other and one cannot live without the help of the other; however, none of the partners suffers any harm from the association.
Commensalism - an association in which the commensal takes the benefit without causing injury to the host. E.g. Most of the normal floras of the humans’ body can be considered as commensals.
Parasitism - an association where one of the partners is harmed and the other lives at the expense of the other. E.g. Worms like Ascaris lumbricoides reside in the gastrointestinal tract of man, and feed on important items of intestinal food causing various illnesses.
EFFECT OF PARASITES ON THE HOST
1. Direct effects of the parasite on the host
Mechanical injury - may be inflicted by a parasite by means of pressure as it grows larger, e.g. Hydatid cyst causes blockage of ducts such as blood vessels producing infraction.
Deleterious effect of toxic substances- in Plasmodium falciparum production of toxic substances may cause rigors and other symptoms.
Deprivation of nutrients, fluids and metabolites -parasite may produce disease by competing with the host for nutrients.
2. Indirect effects of the parasite on the host:
Immunological reaction: Tissue damage may be caused by immunological response of the host, e.g. nephritic syndrome following Plasmodium infections.
Excessive proliferation of certain tissues due to invasion by some parasites can also cause tissue damage in man, e.g. fibrosis of liver after deposition of the ova of Schistosoma.
EFFECTS OF THE HOST ON THE PARASITES
Genetic constitution of the host may profoundly influence the host-parasite relationship (racial variations in resistance to certain strains of Plasmodium vivax; sickle cell trait increased resistance to infection with P. falciparum)
Anti-parasitic immune responses:
Natural immunity– mucocutaneous barrier, blood brain
barrier, phagocyte, complement, defensins…
Acquired immunity
Sterilizing immunity (cutaneous leishmaniasis)
Non-sterilizing immunity– premunition,
concomitant immunity
BASIC & PRINCIPAL CONCEPTS IN MEDICAL PARASITOLOGY
Each of the medically important parasites are discussed under the standard subheadings of:
Morphology;
Geographical distribution/Spreading of the Parasites;
Transmission/means of infection;
Life cycle;
Infection & pathogenesis;
Diagnosis - Clinical & Laboratory diagnosis;
Treatment and
Preventive/control measures of parasites.
Morphology
Includes size, shape, color and position of different organelles in different parasites at various stages of their development.
This is especially important in laboratory diagnosis which helps to identify the different stages of development and differentiate between pathogenic and commensal organisms.
For example, Entamoeba histolytica and Entamoeba coli.
Geographical distribution of the Parasites
Many of them are still found in abundance in the tropics. Distribution of parasites depends upon:
The presence and food habits of a suitable host:
Host specificity, for example, Ancylostoma duodenale requires man as a host where Ancylostoma caninum requires a dog.
Food habits, e.g. consumption of raw or undercooked meat or vegetables predisposes to Taeniasis
Easy escape of the parasite from the host- the different developmental stages of a parasite which are released from the body along with faeces and urine are widely distributed in many parts of the world as compared to those parasites which require a vector or direct body fluid contact for transmission.
Environmental conditions favoring survival outside the body of the host, i.e. temperature, the presence of water, humidity etc.
The presence of an appropriate vector or intermediate host – parasites that do not require an intermediate host (vector) for transmission are more widely distributed than those that do require vectors.
Knowledge of geographical distribution and conditions favoring survival in relation to different parasites, provide effective preventive and control measures
Factors Contributing to Spread of the parasites
Inadequate sanitation and unhygienic living conditions leading to faecal contamination of the environment.
Lack of health education.
Insufficient water and contaminated water supplies.
Failure to control vectors due to ineffective interventions, insecticide resistance, lack of resources, and suspension of surveillance and control measures (e.g. during war and conflict).
Poverty, malnutrition and for some parasites, increased susceptibility due to co-existing HIV infection.
Development schemes introducing opportunities for vector breeding and infection of the workforce, e.g. poorly designed irrigation schemes and dam projects.
Failure of drugs to treat parasitic infections effectively.
Climatic factors.
Population migrations causing poor health, loss of natural immunity, exposure to new infections, and people being forced to live and work closer to vector habitats and reservoir hosts, often in overcrowded conditions, e.g. refugee camps.
Transmission/Means of Infection of the Parasites
Transmission can occur in several ways:
Direct body contact or person-to-person or horizontal transmission - transmission by touching, kissing, sexual intercourse; Vertical transmission: Mother to fetus transmission is important for few parasitic infections like Toxoplasma gondii , Plasmodium spp. and Trypanosoma cruzi.
Blood transfusion: Certain parasites like Plasmodium species, Babesia species, Toxoplasma species, Leishmania species and Trypanosoma species can be transmitted through transfusion of blood or blood products.
Autoinfection: Few intestinal parasites may be transmitted to the same person by reverse peristalsis (internal autoinfection). Ex. Crypto- sporidium parvum, Taenia solium, Enterobius vermicularis, Strongyloides stercoralis and Hymenolepis nana.
Fecal-oral route – can involve direct contact (ex. a person does not wash his hands after defecating and then shakes hands with someone)
Vehicle Transmission (objects such as food, water, fomites) Fomites - inanimate objects such as cups, towels, bedding, eating utensils, bedding, & handkerchiefs
Penetration of the skin and mucous
Vectors -
Mechanical vector
Biological vector
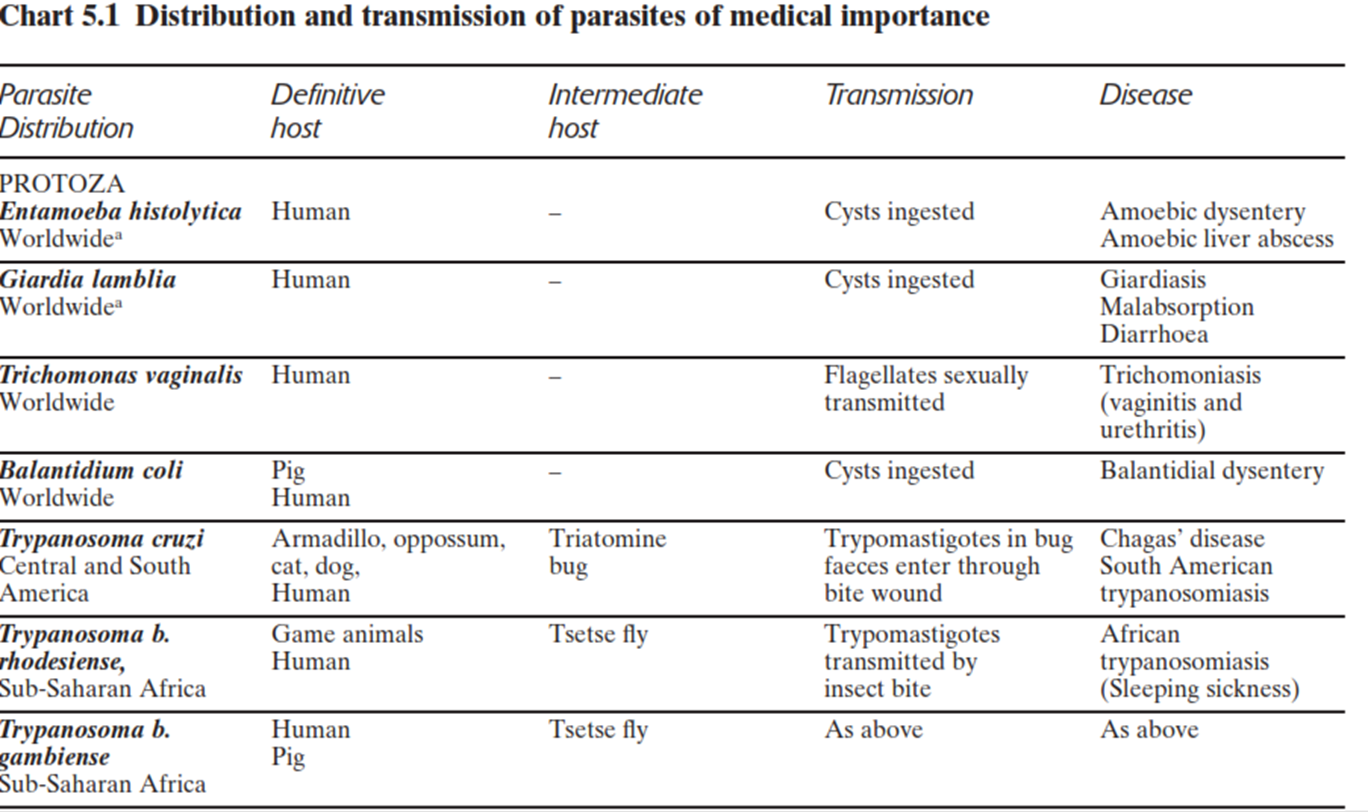
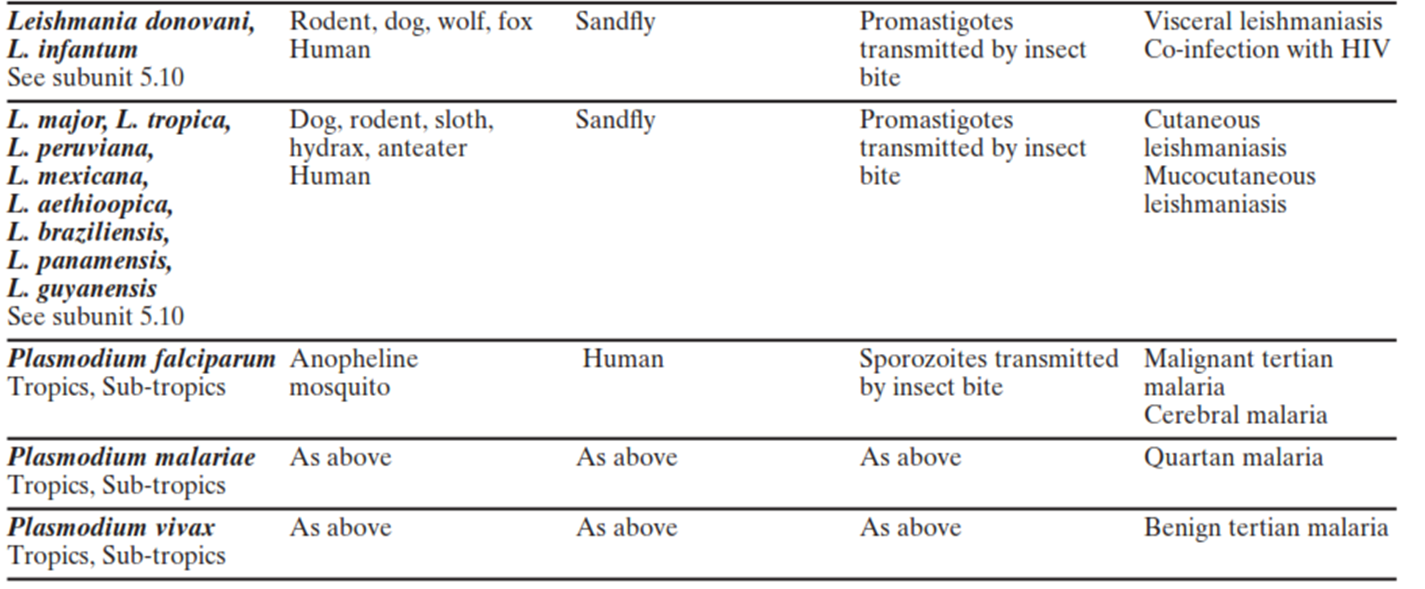
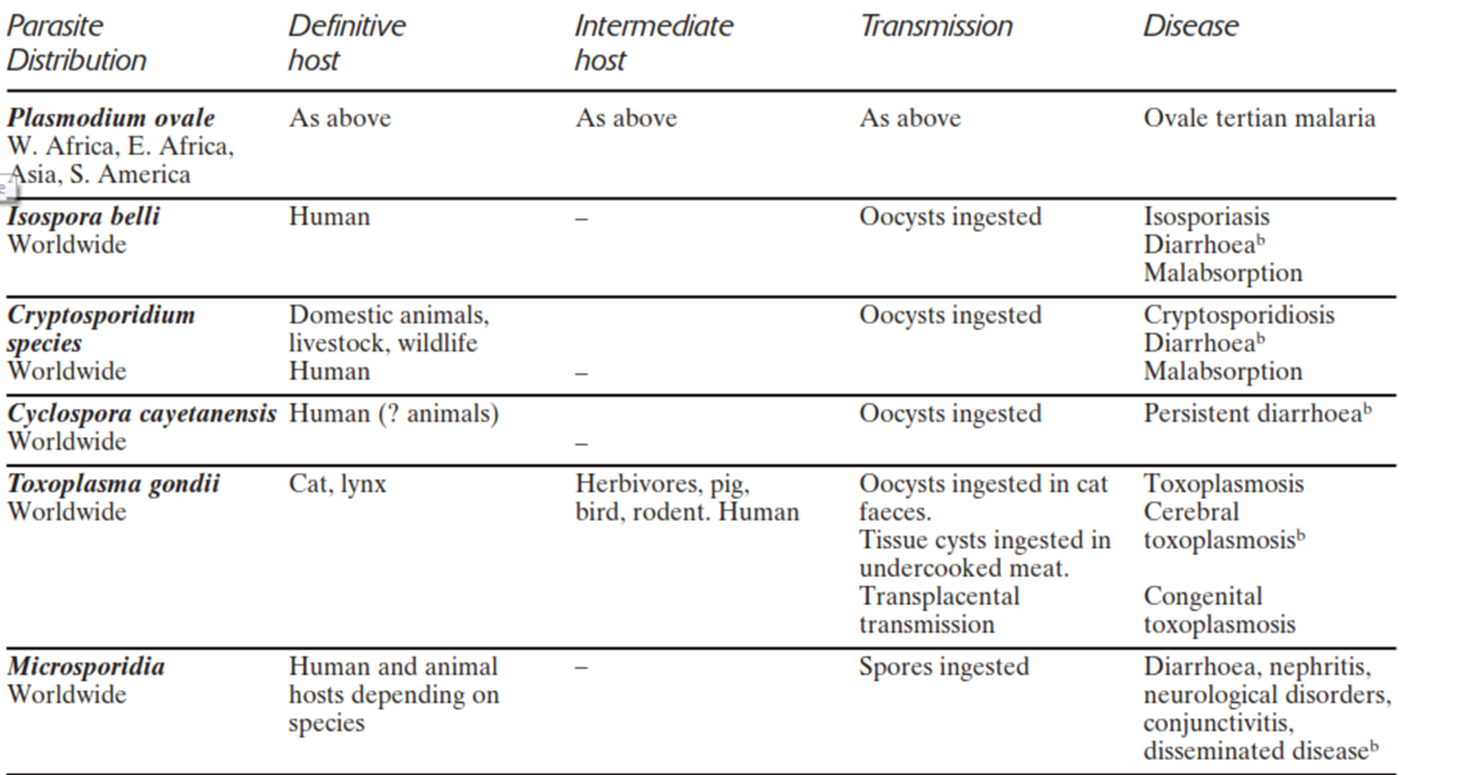
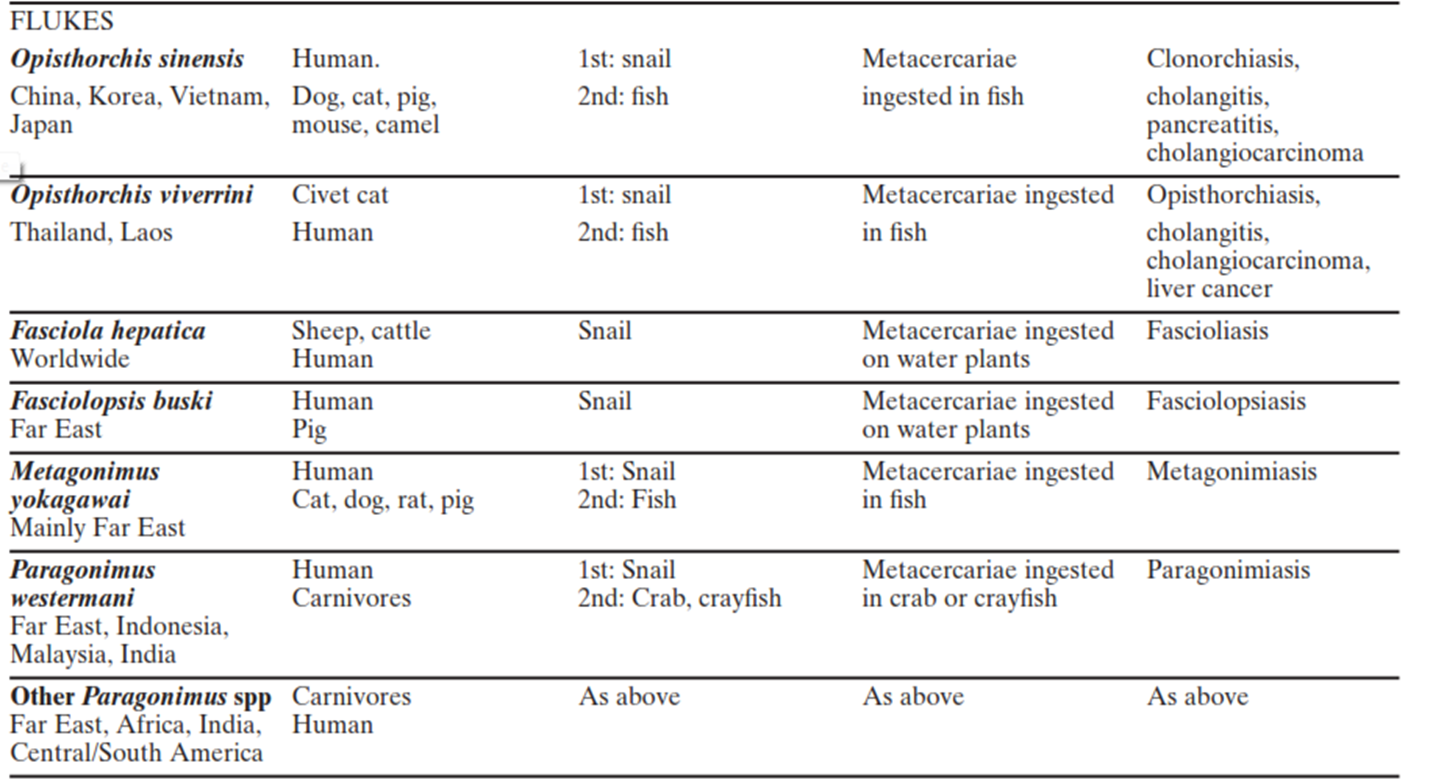
8. Read also chart 5.1 Monica Vol. 1
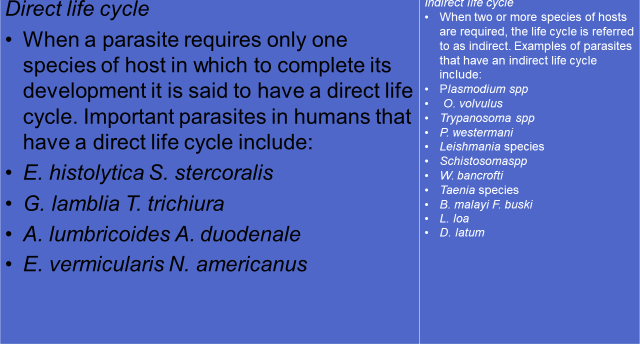
Life cycle of parasites
The route followed by a parasite from the time of entry to the host to exit, including the extracorporeal (outside the host) life.
It can either be simple, when only one host is involved, or complex, involving one or more intermediate hosts.
A parasite’s life cycle consists of two common phases one phase involves the route a parasite follows inside the body. This information provides an understanding of the tissue affected, symptomatology and pathology of the parasite. In addition the method of diagnosis & form of the parasite found in the specimen and selection of appropriate medication may also be determined.
The other phase, the route a parasite follows outside of the body, provides crucial information pertinent to epidemiology, prevention, and control.
Generalized stages of a parasite’s life cycle
Stage in human host (linking to pathogenesis)
Stage to discharge (diagnostic stage)
Stage developing outside human host ( in external environment, intermediate host or insect host)--- (linking to transmission)
Stage infecting men (infective stage)
Infection & Pathogenesis
Infection is the result of entry and development within the body of any injurious organism regardless of its size. Once the infecting organism is introduced into the body of the host, it reacts in different ways and this could result in:
Carrier state - a perfect host parasite relationship where tissue destruction by a parasite is balanced with the host’s tissue repair. At this point the parasite and the host live harmoniously, i.e. they are at equilibrium.
Disease state - this is due to an imperfect host parasite relationship where the parasite dominates the upper hand. It can result either from lower resistance of the host or a higher pathogenecity of the parasite.
Parasite destruction – occurs when the host takes the upper hand.
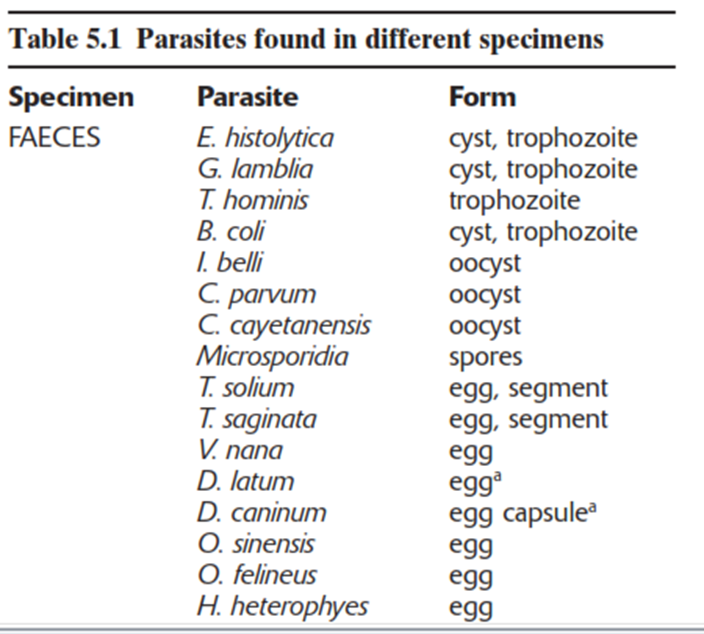
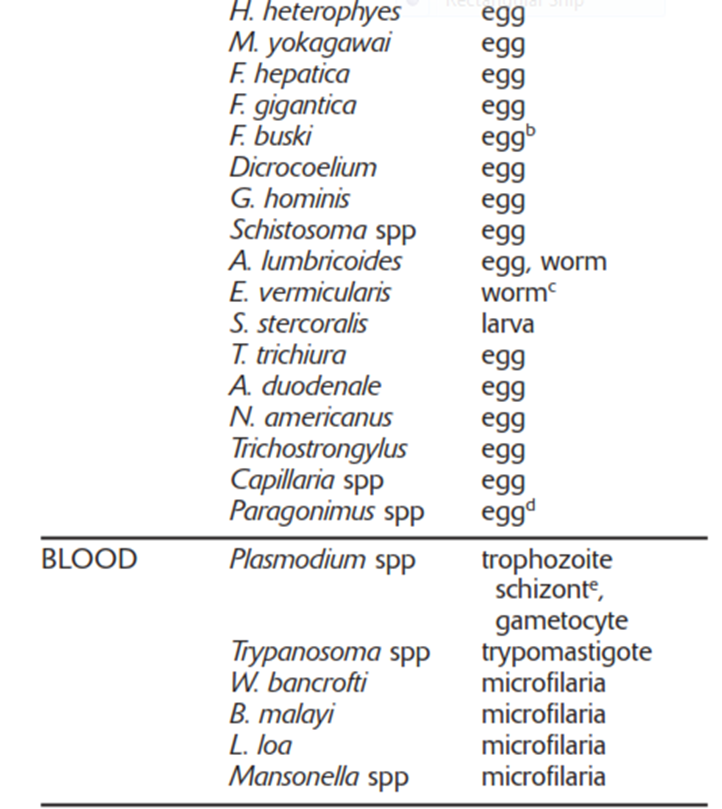
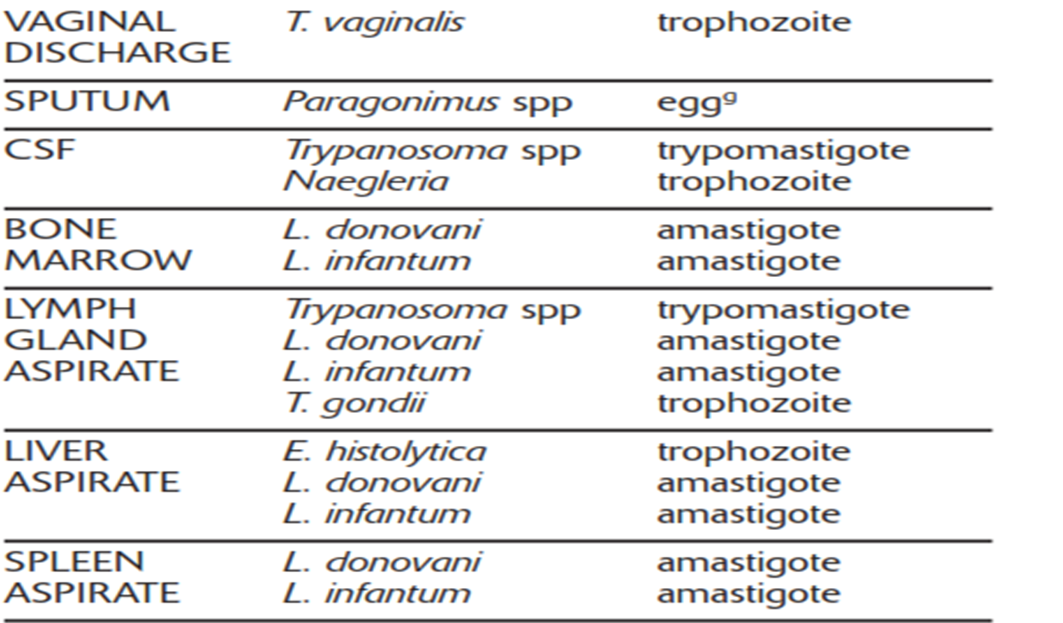
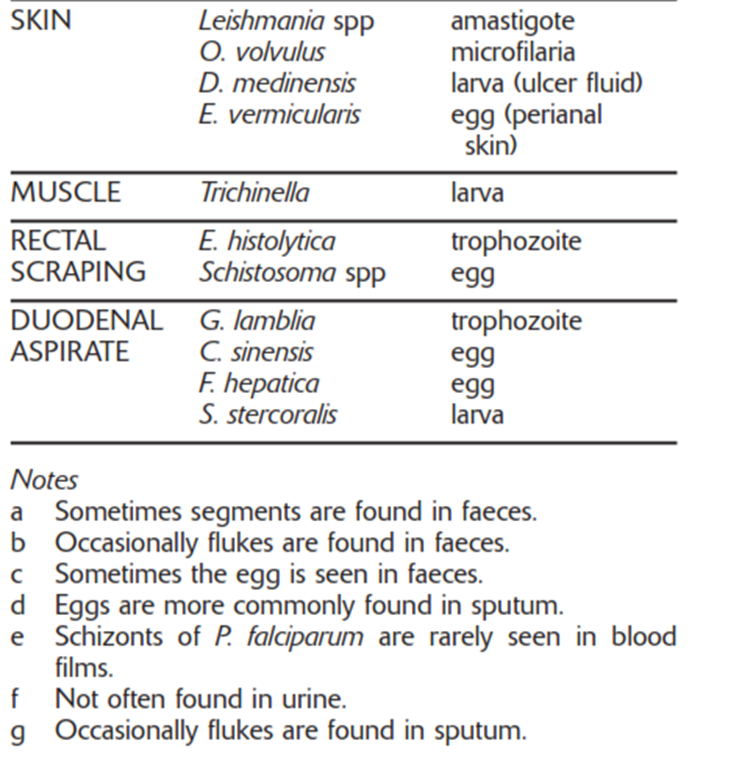
Laboratory diagnosis― Direct Evidences: Ova, cysts, Trophozoites and Adult Worms
Depending on the nature of the parasitic infections, the following specimens are selected for laboratory diagnosis: Read also Table 5.1, Monica Vol 1.
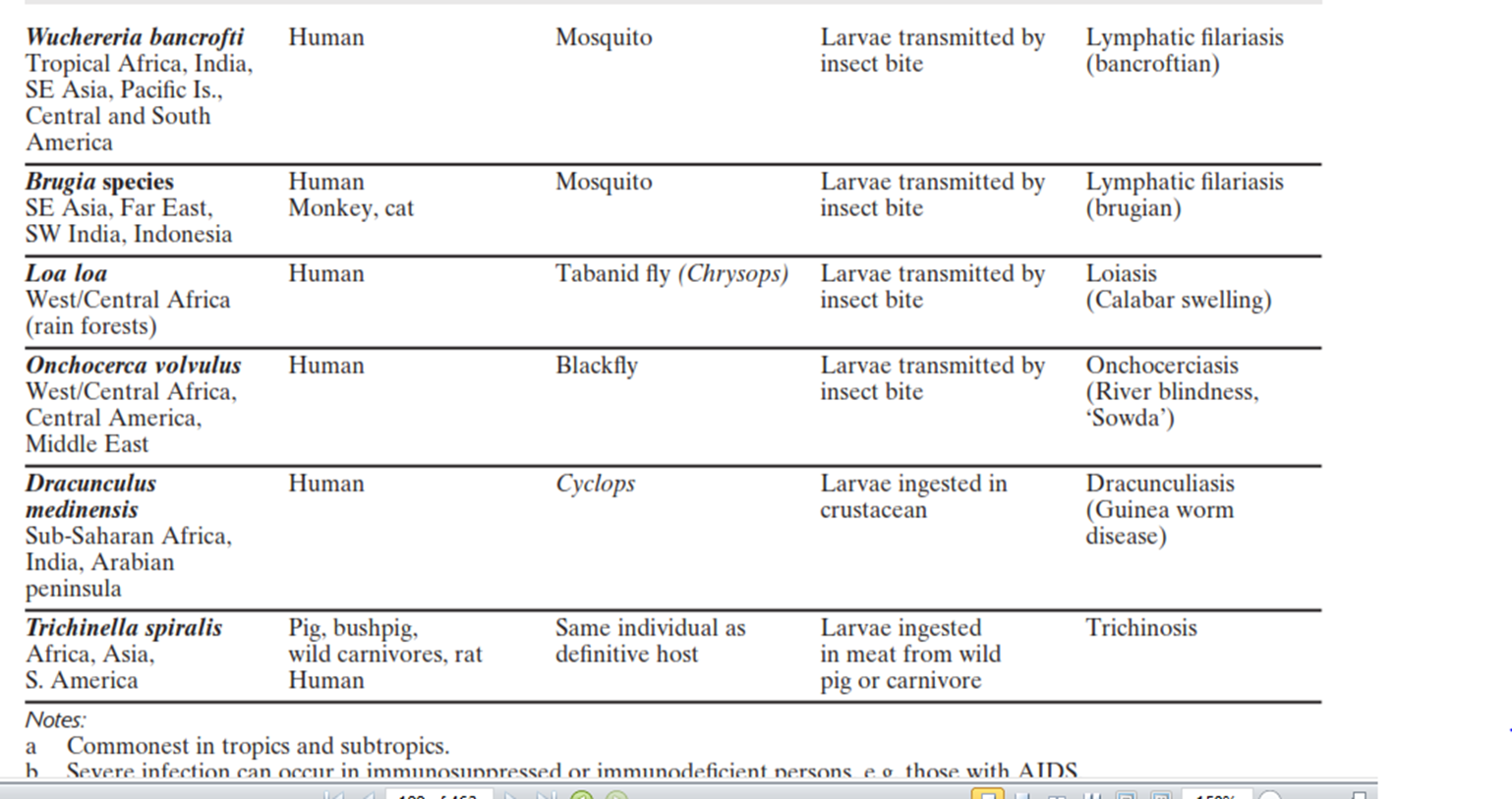
1. Blood – in those parasitic infections where the parasite itself in any stage of its development circulates in the blood stream, examination of blood film forms one of the main procedures for specific diagnosis. For example, in malaria the parasites are found inside the red blood cells. In Bancroftian and Malayan filariasis, microfilariae are found in the blood plasma.
2. Stool – examination of the stool forms an important part in the diagnosis of intestinal parasitic infections and also for those helminthic parasites that localize in the biliary tract and discharge their eggs into the intestine.
In protozoan infections, either trophozoites or cystic forms may be detected; the former during the active phase and the latter during the chronic phase. Example, Amoebiasis, Giardiasis, etc.
In the case of helmithic infections, the adult worms, their eggs, or larvae are found in the stool.
3. Urine – when the parasite localizes in the urinary tract, examination of the urine will be of help in establishing the parasitological diagnosis. For example:
urinary Schistosomiasis, eggs of Schistosoma haematobium are found in the urine.
In cases of chyluria caused by Wuchereria bancrofti, microfilariae are found in the urine.
Trichomnas vaginalis and onchocerca volvulus may also be found
4. Sputum – examination of the sputum is useful in the following:
In cases where the habitat of the parasite is in the respiratory tract, as in Paragonimiasis, the eggs of Paragonimus westermani are found.
In amoebic abscess of lung or in the case of amoebic liver abscess bursting into the lungs, the trophozoites of E. histolytica are detected in the sputum.
5. Biopsy material - varies with different parasitic infections. For example spleen punctures in cases of kala-azar, muscle biopsy in cases of Cysticercosis, Trichinelliasis, and Chagas’ disease, Skin snip for Onchocerciasis.
6. Urethral or vaginal discharge – for Trichomonas vaginalis
Laboratory Diagnosis― Indirect evidences: Cytological changes in the blood and Serological tests
Indirect evidences
Changes indicative of intestinal parasitic infections are:
Cytological changes in the blood – eosiniphilia often gives an indication of tissue invasion by helminthes, a reduction in white blood cell count is an indication of kala-azar, and anemia is a feature of hookworm infestation and malaria
Serological tests – are carried out only in laboratories where special antigens are available.
Treatment – many parasitic infections can be cured by specific chemotherapy.
The greatest advances have been made in the treatment of protozoal diseases.
For the treatment of intestinal helminthiasis, drugs are given orally for direct action on the helminthes.
To obtain maximum parasiticidal effect, it is desirable that the drugs administered should not be absorbed and the drugs should also have minimum toxic effect on the host.
Prevention and control
Measures may be taken against every parasite infectiving humans. Preventive measures designed to break the transmission cycle are crucial to successful parasitic eradication. Such measures include:
Reduction of the source of infection- the parasite is attacked within the host, thereby preventing the dissemination of the infecting agent. Therefore, a prompt diagnosis and treatment of parasitic diseases is an important component in the prevention of dissemination.
Sanitary control of drinking water and food.
Proper waste disposal – through establishing safe sewage systems, use of screened latrines, and treatment of night soil.
The use of insecticides and other chemicals used to control the vector population.
Protective clothing that would prevent vectors from resting in the surface of the body and inoculate pathogens during their blood meal.
Good personal hygiene.
Avoidance of unprotected sexual practices.
Michael O Harhay, John Horton & Piero L OlliaroEpidemiology and control of human gastrointestinal parasites in childrenExpert Rev Anti Infect Ther. 2010; 8(2):219-234
CLASSIFICATION OF MEDICALLY IMPORTANT PARASITES
OVERVIEW-Classification of organisms
2 major types of organism
1. Acellular are–
“without a cell” (viruses, prions and viroids)
2. Cellular are-
Prokaryotic ("before nucleus") – these are cells, but they have no internal membrane bound structures (no membrane-bound nucleus or membrane-bound organelles); includes only the bacteria.
Eukaryotic ("true nucleus") – do have internal membrane bound structures (membrane bound nucleus and membrane-bound organelles); includes organisms such as protozoans, fungi, algae, animals, plants.
No single classification system is completely accepted by all biologists, but one of the most widely accepted is the five-kingdom system for the cellular organisms.
Kingdom Monera
Kingdom Protista
Kingdom Fungi
Kingdom Plantae
Kingdom Animalia
The 6 major groups of microorganisms:
viruses,
bacteria,
algae,
fungi,
protozoa, and
Helminthes (worms)
Important Note: While most of the adult stages of these worms are macroscopic, many of them go through a microscopic stage in their life cycles (egg & larval stages), thus grouped as microorganisms.
CLASSIFICATION OF MEDICAL PARASITES SUMMARY
Parasites of medical importance come under the kingdom called protista and animalia.
Protista includes the microscopic single-celled eukaroytes known as protozoa.
In contrast, helminthes are macroscopic, multicellular worms possessing well differentiated tissues and complex organs belonging to the kingdom animalia.
Medical Parasitology is generally classified into:
Medical Protozoology - Deals with the study of medically important protozoa.
Medical Helminthology - Deals with the study of helminthes (worms) that affect man.
Medical Entomology - Deals with the study of arthropods which cause or transmit disease to man
Artificial & Natural Systems of Classification of Organisms
1. Artificial - the Linnaean scheme; he grouped organisms on the basis of visible similarities, but does not indicate how closely organisms are related.
2. Natural - based on evolutionary (phylogenetic) relatedness.
Super class Super family
↑ ↑
Phylum→Subphylum→Class→order→Family→Genus→Species
↓ ↓
Subclass Subfamily
3. For practical diagnostic purposes Artificial approach is preferred.
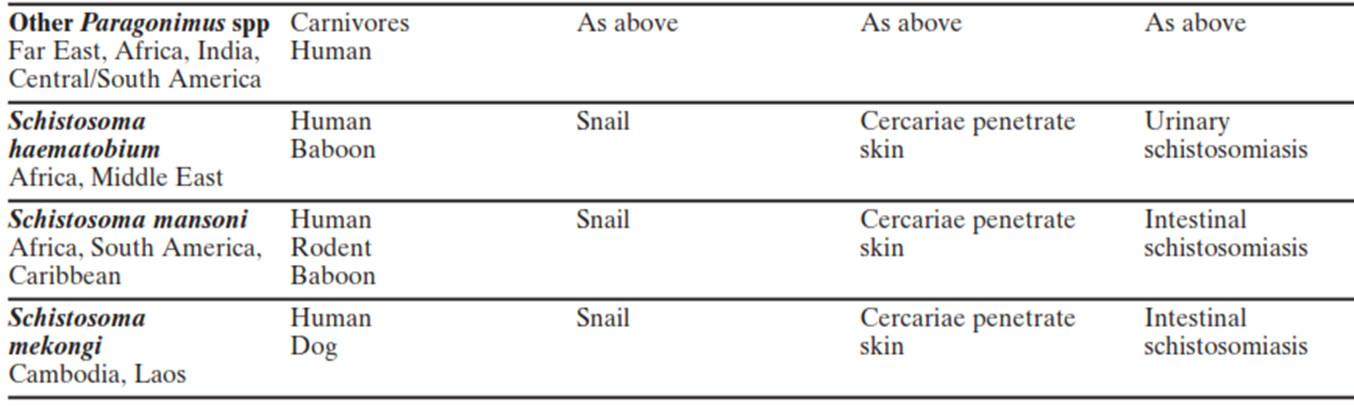
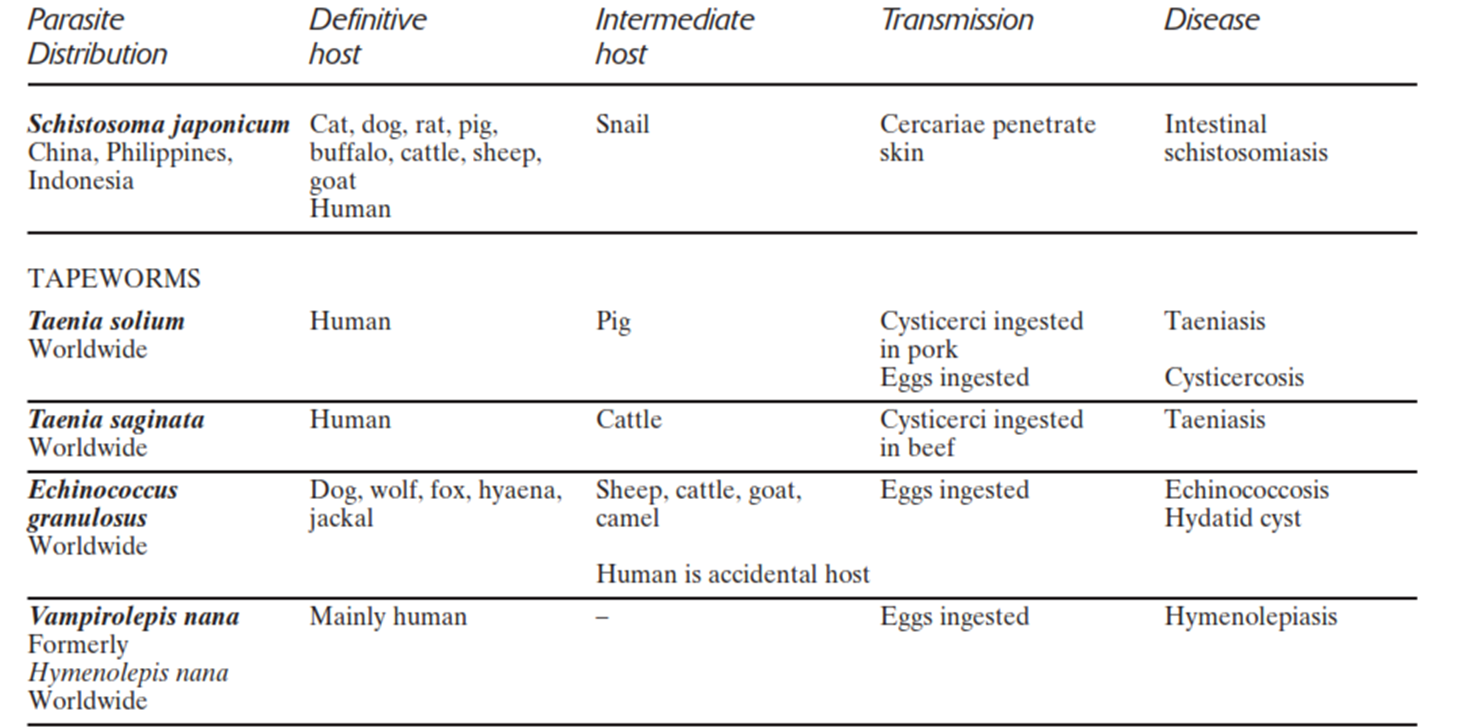
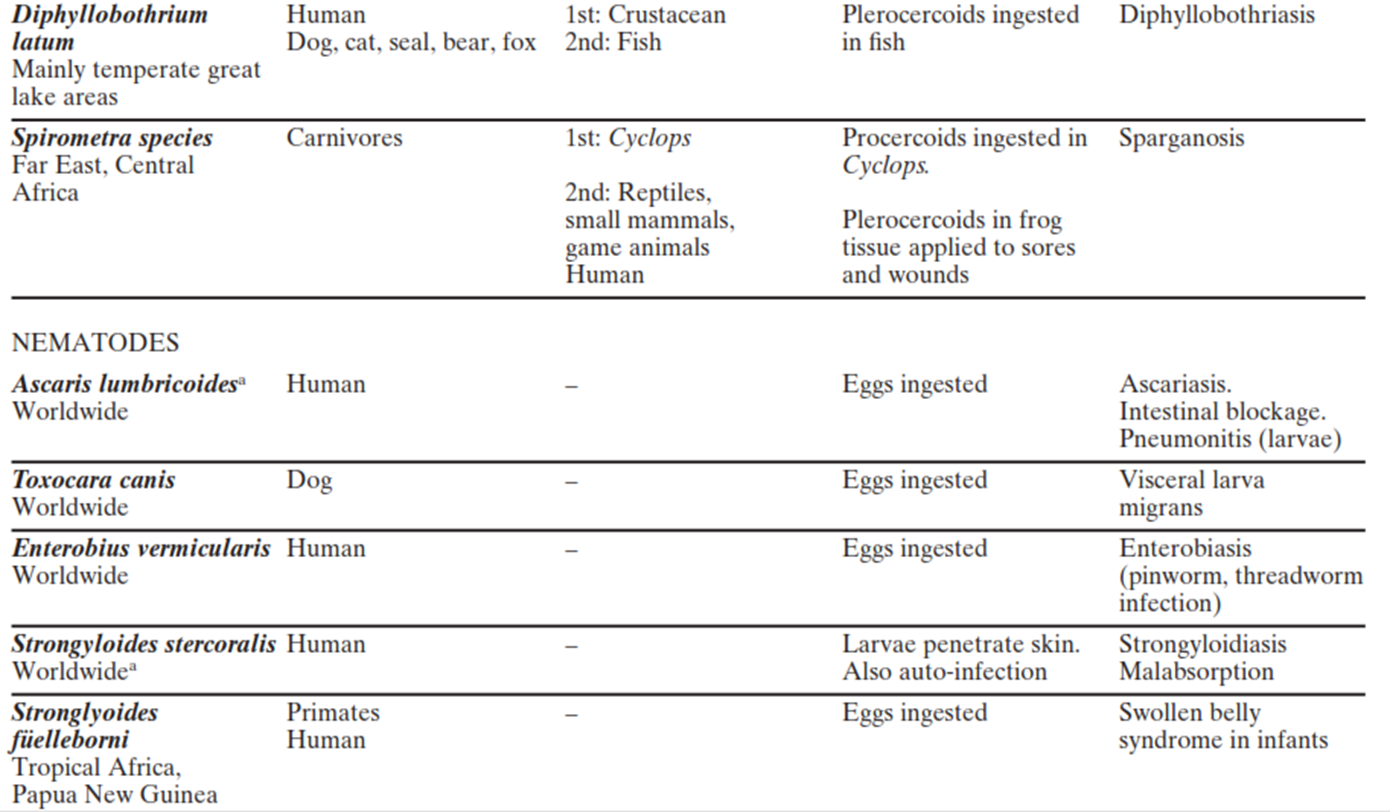
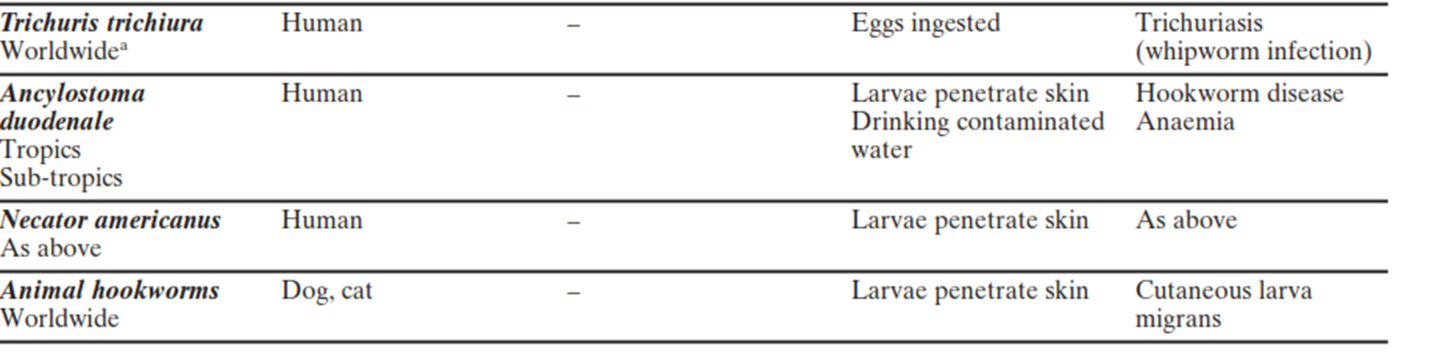
TABE: PRACTICAL CLASSIFICATION OF PARASITES OF MEDICAL IMPORTANCE
|
PROTOZOA |
METAZOA (HELIMINTHS) |
|
1. Sarcodina (Amoebae): (i) Genus, Entameba: E.g. Entameba histolytica (ii) Genus Endolimax E.g. Endolimax nana (iii) Genus Iodameba E.g. Iodameba butchlii (iv) Genus Dientmeba E.g. Dientameba fragilis (v) Acanthamoeba species (vi) Naegleria species |
1. Platyhelminthes: |
|
a)Trematodea
(Flukes): (i) Genus Fasciola E.g. F. hepatica (ii) Genus Schistosoma (viii) Heterophyes heterophyes (ix) Dicrocoelium dendriticum
E.g. S. mansoni (iii) Genus Paragonimus (iv) Fasciolopsis buski (v) Opisthorchis (Clonorchis) sinensis (vi) Opisthorchis viverrini Lesser medical importance: (vii) Metagonimus yokagawai |
|
PROTOZOA |
METAZOA (HELIMINTHS) |
|
2. Mastigophora (Flagellates) i.Giardia lamblia
ii.Trichomonas vaginalis
iii.Trypanosoma species
iv.Leishmania species
|
1. b. Cestoda: (Tapeworms) i.Echinococcus granulosus (larvae)
ii.Taenia species
iii.Diphyllobothrium latum
iv.Hymenolepis nana
v.Vampirolepis nana (less important)
vi.Spirometra spicies
|
|
3. Ciliates Balantidium coli |
|
|
4. Sporozoa (Coccidia) Blood and tissue coccidia: i.Plasmodium species
ii.Toxoplasma gondii
iii.Intestinal coccidia:
iv.Isospora belli
v.Cryptosporidium parvum
vi.Cyclospora cayetanensis
|
|
|
2. Nemathelminthes: (Round worms) a. Intestinal nematodes: i. Ascaris lumbricoides (large roundworm) ii. Hookworms iii. Enterobius vermicularis iv. Strongyloides species v. Trichuris trichiura |
|
|
5. Microsporidia i.Encephalitozoon species
ii.Enterocytozoon species
|
|
PROTOZOA |
METAZOA (HELIMINTHS) |
|
b. Filarial and other tissue nematodes: i.Wuchereria bancrofti,
ii.Brugia species,
iii.Loa loa,
iv.Onchocerca volvulus
v.Drancunculus medinensis (Guinea worm),
vi.Trichinella species
vii.Toxocara canis
viii.Animal hookworms
ix.Trichinera spiralis
|
|
GENRAL CHARACTERISTICS FOR PROTOZOA
Unicellular eukaryotes.
The protistan lineages continue into the kingdoms of plants, fungi, and animals.
Lack a cell wall and therefore limited to a moist environment
Heterotrophs
Most reproduce asexually by fission (one cell divides to form 2 identical daughter cells & budding; some (ex. Plasmodium that causes malaria) undergo schizogony (multiple fission). Sexual reproduction occurs by conjugation, the fusion of vegetative cells, or by the fusion of specialized gametes called gametocytes.
Some have complex life cycles, requiring multiple hosts and changing their morphology (ex. Plasmodium uses the mosquito as an intermediate host)
Trophozoite - active, motile, feeding stage of protozoans; parasitic stage that causes the disease in the host.
Cyst - resistant, inactive stage; usually more useful than trophozoites for lab identification.
Diseases: transmitted by the fecal-oral route of contaminated food and water; or Insect bit inoculums or rubbing on the bit & sexual intercourse
Factors that are important for pathogenecity include:
• Attachment to the host tissue followed by replication to establish colonization.
• Toxic products released by parasitic protozoa.
• Shifting of antigenic expression to evade the immune response and inactivate host defences.
GENRAL CHARACTERISTICS FOR Mastigophora
Move by means of flagella
Trypanosoma gambiense - infects the blood and tissue fluids; causes African sleeping sickness (it leads to the loss of consciousness and death when it invades the CNS); can also infect cattle; vector is the tsetse fly.
Giardia lamblia - body has the appearance of a human face (4 “eyes” are nuclei); have 2-6 flagella; form cysts; causes a waterborne dysentery (traveler's diarrhea); one of the “don’t drink the water” diseases; firs sigh is usually an explosive, foul-smelling watery diarrhea followed by copious amounts of campers are a high-risk group because of asylvatic cycle (parasite is found in mountain streams contaminated with human feces or animal feces, especially beavers).
Trichomonas vaginalis - causes vulvovaginitis; numerous flagella
GENRAL CHARACTERISTICS FOR Sarcodina
Move by means of pseudopodia or "false feet" - temporary extensions of the cell body caused by protein filaments of the cytoskeleton pushing on the cell membrane); feed on algae, bacteria, and other protozoans by phagocytosis.
Amoeba proteus - freshwater; not pathogenic
Entamoeba histolytica - causes amoebic dysentery; usually acquired by consuming fecally contaminated water or food; flies and cockroaches can also be mechanical vectors; produce cysts; first protozoan to be shown to be a pathogen (1875); one of the “don’t drink the water” diseases; trophozoites may invade the intestinal mucosa where they can cause ulceration and escape into the blood vessels; they may allow bacteria in fecal material to enter the body cavity and cause peritonitis.
Naegleria fowleri - causes amoebic meningioencephalitis; usually seen in swimmers.
Acanthamoeba polyphaga – accumulates on the water surface of contaminated hot tubs when tubs are covered; cause ulceration of the eyes and skin; can invade the central nervous system and cause meningioencephalitis.
GENRAL CHARACTERISTICS FOR Ciliophora
Move by means of cilia
Paramecium caudatum - freshwater; not pathogenic
Balantidium coli - only ciliophoran that causes disease; produces cysts; causes diarrhea of large intestine; rare except in the Philippines; symptoms are similar to those of amoebic dysentery.
GENRAL CHARACTERISTICS FOR Sporozoa
Basically nonmotile.
All have an infectious, sporelike stage (sporozoite) that is often transmitted to new hosts by an insect vector.
All are parasitic (obligate parasites - cannot live apart from the host).
Some have elaborate life cycles, changing body form (trophozoite, sporozoite, merozoite); life cycle includes schizogony (multiple fission). Examples
Plasmodium vivax - causes malaria; vector is the mosquito; kills 1-3.5 million people each year; malaria = bad air; used to infect people with malaria to stop the progression of syphilis (fevers would kill the bacteria).
Toxoplasma gondii- causes toxoplasmosis; humans acquire the disease by consuming cysts in the meat of infected animals or ingesting material contaminated by cat feces containing the parasite (can get it from cleaning the litter box - doctors warn pregnant women not to do this).
Cryptosporidium - form cysts; cause enteritis & diarrhea; can occur in water supplies; can also be transmitted by fecal-oral transmission from kittens/puppies; resistant to chlorine (it can survive full-strength Chlorox!); threat only AIDS patients and those immunocompromised; no effective treatment found.
Pneumocystis carinii - may be a fungus!!; causes pneumocystis pneumonia; spread in respiratory droplets; common in AIDS patients.
GENRAL CHARACTERISTICS FOR Microsporidia
Microsopridia are obligate intracellular spore-forming microorganisms,
normally pathogenic in fish, insects, and other invertebrates and mammals.
In humans they have been reported as pathogens in those infected with HIV.
In host cells, there are successive cycles of schizogony (merogony) followed by sporogony from which many spores are produced.
GENRAL CHARACTERISTICS FOR HELMITHES
Animals
Cephalization - concentration of sensory receptors toward the anterior end.
Organ/system level or organization/
Sexual reproduction. Most flatworms are monoecious (male & female reproductive organs in same animal). Roundworms are dioceious (separate sexes).
General Xtics Platyhelminthes (Flatworms = Trematodes + Cestodes)
Flat worms
most are free-living; marine and freshwater; predators, scavengers, or parasitic;
Some have regenerative capabilities.
General Xtics of Trematoda (Flukes)
Shape: Leaf like (except Schistomes) and unsegmented
Head end: Sukers no hooks
Sexes: Not separate, (monoecious) Except blood flukes (Schistosomes) which are dioecious
Alimental canal: Present but incoplete
Body cavity: Absent
all parasitic of vertebrates; in blood venules around the gut or bladder, Lungs and small intestines, biliary tract
have complex life cycles that include sexual and asexual phases; they require at least 2 kinds of organisms to complete the cycle - they reach sexual maturity in a primary or definitive host (always a vertebrate), their larval stages develop or become encysted in an intermediate host (usually an invertebrate).
General Xtics- Cestoda (Tapeworms)
Morphology: Tape-like and segmented : scolex (head) with suckers and/or hooks (for attachment), proglottids (body units - each one has male and female reproductive organs (monoecious): immature proglottids (closest to the scolex), mature proglottids (next closest to the scolex), and gravid proglottids (furthest from the scolex - in these proglottids, the uterus is filled with eggs).
Alimental canal: Absent
Body cavity: Absent
intestinal parasites of humans (With the exception of E. granulosus, the dog tape worm whose larvae (hydatid cysts live in lungs, liver and brain of humans); no digsetive system like in trematodes & nematodes; they absorb nutrients through their tegument!
General life cycle of tapeworms: the gravid proglottids break off and are passed in the definitive host's feces; larval forms hatch when the eggs are ingested by the intermediate host; larvae then encyst in the intermediate host (called a cysticercus or bladder worm); adult worms usually develop in the definitive host when raw or poorly cooked infected meat is eaten.
General Xtics of Nematodes
Shape: Elongated and cylindrical
Head end: No Sukers and hooks
Sexes: Dioecious (separate sexes).
Alimental canal: Present and complete
Body cavity: Present
Nematodes are everywhere!!!! They are freeliving in soil, fresh & salt water, & are parasitic in plants and animals
Possess a nonliving cuticle, which is secreted by the epidermis and is resistant to the digestive enzymes of the hosts.
More highly developed than flatworms.
Adults do not hatch into the host like the tapeworms.
Females are either viviparous (produce larvae) or oviparous (lay eggs).
LINE BASIC DIAGNOSTIC TECHNIQUES IN THE MEDICAL PARASITOLOGY LABORATORY
OUTLINE
Microscope and Microscopy
Microscopy overview
Proper use and care of the microscope
Commonly Used Diagnostic Techniques
Preparation of patient
Collection of faecal sampels for parasitical tests
Preservation of samples for parasitical tests
Direct examination of faecal samples
Concentration techniques for faecal samples
Permanent stains, preparation of smears and staining
Reporting test results
MICROSCOPE & MICROSCOPY
Outline:
Overview of microscopy
Use and care of a light microscope
Microscopy Overview
Microscopes are essential tools for microbiological studies.
Microscopy is the technology of making very small things visible to the human eye. Most microbes are so small that they are measured in micrometers or nanometers.
Two types of microscopes
Light microscopes: cellular resolution
bright-field (stains)
dark-field
phase contrast
fluorescence (stains)
Electron microscopes: subcellular resolution
Optics
Principles
Resolution is the ability to see two objects as separate, discreet entities….kind of like the ability to see railroad tracks as being separate tracks….GOOD resolution is being able to distinguish the two tracks as separate…..once the two tracks merge into one, the resolution is poor!!!
Refraction is the bending of light as it passes from one medium to another of different density. Immersion oil, which has the same index of refraction as glass, is used to replace air and to prevent refraction at a glass-air interface. An example would be when one looks at objects just below the surface of water in a pond or other body of water…..the objects become refracted or “distorted” from the true image.
Visualization depends on magnification (lenses) and resolution (physical properties of light)
The limit of resolution for a light microscope is about 0.2 micrometers (or 200 nm)
Objects closer than 0.2 micrometers cannot be resolved
Total magnification is product of the magnification of its ocular and its objective lenses
Useful magnification is the range of total magnifications within which details in the object are seen clearly in the image
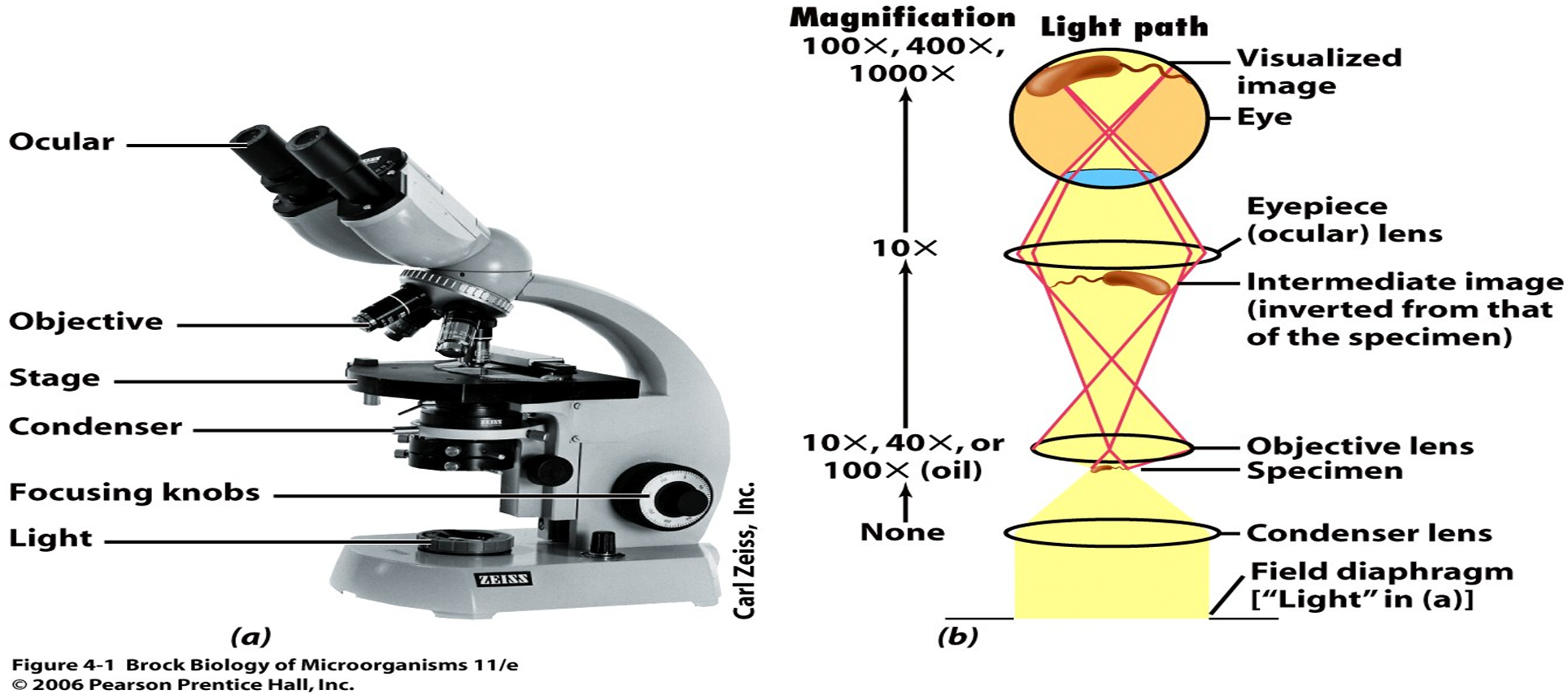
Image: Microscope and its Optical System
Microscopy
Scanning (3X) x (10X) = 30X total
Low power (10X) x (10X) = 100X total
High “dry” (40X) x (10X) = 400X total
Oil immersion (100X) x (10X) = 1000X total
Most microscopes are designed so that when the microscopist increases or decreases the magnification by changing from one objective lens to another, the specimen will remain very nearly in focus.
Summary of how to use a microscope with built-in illumination
Position the microscope correctly and identify the essential parts.
Before switching on the microscope turn the lamp brilliance control to its lowest setting, then increase it to about three quarters of its power.
Bring the 10 objective into place.
Make sure the underside of the specimen slide and surface of the stage are completely dry and clean.
Place the specimen on the stage in the slide holder.
Focus the specimen with the 10 objective.
Focus the condenser (should be within 1mm of its topmost position) and leave it in this position for all objectives.
If the microscope is not fitted with a pre-centered condenser, check the centering of the condenser.
Examine the specimen with the 10 objective. Obtain the best image by:
– closing the iris about two thirds,
– adjusting the lamp brightness control to give good illumination with the minimum of glare.
Use the mechanical stage to examine the specimen systematically.
Examine the specimen with the 40 objective. Obtain the best image by:
– opening the iris more,
– increasing the illumination.
Examine the specimen with the 100 objective. Move the 40 objective to the side, place a drop of oil on the specimen and bring the 100 objective into position. Obtain the best image by:
– opening the iris fully,
– increasing the illumination.
To prevent damage to the 100 objective lens, move the objective to one side before removing the specimen.
CARE OF THE MICROSCOPE
DO’s
Do keep the microscope covered with a clean plastic or cloth cover when it is not in use
Do keep special care to protect the microscope from dust in hot dry periods
Do take special care to protect the microscope lenses and prisms from fungal growth in hot humid period. This can be done by:
Keeping the microscope in air conditioned room or
Storing the microscope in special dehumidified room or
Connecting a number of bulbs of 15 to 25 watts inside a cupboard with tightly fitting doors
Do clean immersion oil from the immersion objective every day; use a soft cloth damped with ethanol/ether (3ml/7ml) or benzene/ethanol/ether(2ml/2ml/1ml) and polish with a clean, lint-free cloth;
an altanative, use lens tissue or facial tissue, if available.
Do clean the oculars with a soft, lint-free cloth; as an alternative, use lens tissue or facial tissue, if available.
Do use the microscope retaining screw fitted at the base of the microscope box to prevent damage to the instrument during transit
Do quote the model number and, if possible, the instrument and part number when ordering the replacement parts.
CARE OF THE MICROSCOPE
DONT’s
Don’t use the tissue or cloth used for the oil immersion objective to clean the oculars.
Don’t use alcohol to clean painted surfaces of the microscope
Don’t dismantle or try to clean parts of the microscope that are difficult to reach, unless you have been trained to do so.
Don’t leave the lens ports empty; use the appropriate cover or some sticking plaster to cover the empty port.
Don’t exchange lenses from microscopes of the different manufactures even some models by the same manufacturers have different specifications
THE COMMONLY USED BASIC DIAGNOSTIC TECHNIQUES IN THE MEDICAL PARASITOLOGY LABORATORY
1. Preparation of patient
2. Sample Collection/Handling and Preservation Methods
3. Wet mount Preparation
Normal saline 0.85%
Iodine
BMB
4. Artifacts
CONCENTRATION TECHNIQUES
5. Modified Formal- Ether Sedimentation technique
For larvae, ova and cysts
For oocysts
6. Acid- Ether Sedimentation technique
7. Flotation Techniques
By using Sheather’s solution
By using Sodium Chloride solution
By using Zinc Sulphate
8. Staining of parasites
9. Detecting of Blood Parasites
Thick and
thin Blood smear
10. Counting of Helminthes Eggs in Feces
11. Chemical Tests
Fecal PH test
Testing feces for Occult Blood
Fecal fat test
Stool reducing sugar test
What is the stool or feces?
Waste residue of indigestible material
Bile pigments and electrolyte.
Intestinal secretions, including mucus.
Leukocytes that migrate from the bloodstream
Epithelial cells that have been shade.
Bacteria and Inorganic material(10-20%) chiefly calcium and phosphates. Undigested and unabsorbed food
Fecal Specimen
Fecal specimen are examined for protozoa, helminthes larvae or eggs.
The stages of protozoa found in stool samples are trophozoites and cysts or oocysts.
The stages of helminths usually found in the stool samples are eggs and larvae, though whole adult worms or segment of worms may also be seen.
Adult worms and segment of tape worms are usually visible to naked eye, but eggs, larvae, cyst, oocyst and trophozoites can be seen only with the microscope.
In order to see these structure, the fecal material must be properly collected and examined.
Number of Specimens and Collection Time
No technique is 100% successful in detecting parasites by single stool examination, and at least three serial stools must be examined before a patient can be considered free from infections in which stages of parasites would be expected to be free in the faeces.
Because of the intermittent passage of certain parasites, the possibility of finding organisms is increased by examining multiple specimens.
It is suggested that 3 specimens, collected at 2 to 3 day intervals, should be examined both pretreatment and post treatment (to ensure eradication of documented pathogenic protozoa).
Illustration of Collection and Handling of Sample by/of Fecal Specimen
Because of fragile nature of many intestinal parasites, and the need to maintain their morphology for accurate identification.
Reliable microscopic diagnosis can not made unless the stool is collected properly.
The stool specimen must be enough for satisfactory examination of fresh feces uncontaminated by urine, dirt*, water or other body secretion such as menstrual blood.
If the sample is too small or contaminated with urine, it should not be accepted. Ask the patient to pass another specimen.
Collect the specimen in a clean dry screw-capped top container
Collect the stool with a clean tongue blade or similar object.
The container should be free from antiseptics and disinfectant.
Random specimen: suitable for qualitative testing for blood and microscopic examination.
Timed specimen: for quantitative fecal testing such as fecal fat testing, because of the variability of bowel habit and the transit time required for food to pass through the digestive tract, so the most representative sample is a-3 day collection.
The container with the specimen should be clearly labeled with the following:
Patient’s name and/or number.
Date and time of collection.
All samples should be accompanied by a requisition form from the physician giving relevant clinical details and recent travel history.
Samples and forms from patient with a confirmed or suspected diagnosis of certain infectious diseases such as AIDS or hepatitis should be clearly labeled with “Biohazard”
Most viable parasites are susceptible to desiccation or temperature variation.
If time lapse between collection and observation is considerable, i.e. more than 4 days, it may be necessary to add some form of preservative to feces specimen to retain morphology.
Formed samples can be kept in a refrigerator at 4 C° for a short time, but not in incubator.
Any whole worms or segments passed should be placed in a separate container
Preservation methods for fecal specimens
Preservation allows fecal samples to be examined after a delay in delivery or postage or testing.
Many methods for the preservation of stool samples and permanent staining procedures.
The most common fixatives are:
Polyvinyl Alcohol, PVA
Merthiolate Iodine Formalin, MIF
Sodium acetate Acetic acid Formalin, SAF
Formalin.
Bayer’s solution*
The preservatives used have different effect on the various stages of the parasites.
Formalin
Formalin 4% has been used for many years as an all purpose fixative that is appropriate for helminthes eggs and larvae and for protozoan cyst.
The fixative has a long shelf life.
Concentration methods, like formalin- ether concentration can be performed from the preserved stool samples without loss of concentration abilities.
The major disadvantage of formalin is that permanent staining procedures can't be performed from formalin preserved stool samples.
PVA
This fixative is recommended for the preservation of the trophozoite and cyst stages of the intestinal protozoa, and also suitable for helminthes eggs and larvae.
The preservation of the two stages of protozoa is excellent.
The PVA is a plastic resin that serves as adhesive for the stool material.
Has a long shelf life. ( months to years ).
Concentration methods can’t performed from the specimen preserved by PVA.
The greatest advantage of this fixative is that a permanent stain can be prepared from stool specimen preserved by PVA, giving excellent result with trichrome staining.
Specimen preserved by PVA can’t be used with immunoassay kits.
Toxic, because contain mercury compound.
SAF
Good routine fixative for protozoan cyst and trophozoites, helminthes eggs, and larvae.
Has long shelf life. ( months to years).
The preserved stool samples permits concentration techniques, most monoclonal detection kits, and permanent staining.
Unlike the PVA, the SAF fixative has poor adhesive properties when SAF preserved samples are used to prepare permanent stained smears. ( Mayer’s albumin has been recommended as an adhesive.
The combination of SAF preserved material and CB, IHK, and mod. Ziel Neelsen provides excellent staining of protozoan where staining of SAF preserved material with Trichrome gives poor results.
Specific advantages of the use of SAF are:
SAF preserved material can be used for concentration techniques and permentant stained smears (CB, IHK).
SAF preserved material can be used for some immunoassay methods.
SAF is easy to prepare and has a long shelf life.
Unlike the PVA, the SAF fixative contain no mercury compounds. It is therefore much less toxic than PVA
MIF
This fixative was originally developed as a screening procedure for intestinal parasites.
MIF combines preservation and staining for most kinds and stages found in faeces.
It’s contains Merthiolate, Iodine, and Formalin.
The preserved material permits concentration techniques.
The major disadvantages are the short shelf life ( duo to iodine) and permanent stained smears can’t be prepared from MIF preserved material.
Fixative used for the preservation of stool samples: an overview of the advantages and disadvantages:
|
Formalin 4% |
PVA |
SAF |
MIF |
|
|
Toxicity |
+/- |
+++ ( duo to Hg ) |
+/- |
+/- |
|
Shelf life |
Long (months) |
Long (months/years) |
Long (months/years) |
Limited |
|
Preparation |
Easy |
Difficult |
Easy |
Easy |
|
Quality of fixation |
Egg: ++ |
Egg: ++ |
Egg: ++ |
Egg: ++ |
|
Cyst: ++ |
Cyst: +++ |
Cyst: ++ |
Cyst: ++ |
|
|
Troph’s: +/- |
Troph’s: +++ |
Troph’s: +++ |
Troph’s: +/- |
|
|
Formalin ether concentration |
Possible |
Not possible |
Possible |
Possible |
|
Permanent stained smear |
Not possible |
Only Trichrome |
IHK, CB, mod. Ziel Neelsen |
Not possible |
Preservation of worms
Cestodes
Wash in water to remove the mucus. Large tapeworms such as Taenia can be washed for several hours to relax the musculature, and can then be fixed in 10% formol saline b/w two glass slides to give flatter specimens.
Trematodes
These should be treated in a similar manner to cestodes, and mounted with the ventral sucker uppermost
Nematodes
Adult are washed in saline to remove mucus. Worms up to about 7 cm in length are fixed in hot(60-70˚C) 70% alcohol, which straightens out living worms, except those which have natural curvatures at the head or the tail. Alternatively, they can be fixed in hot 5% formalin.
Large worms such Ascaris lumbricoides can be fixed and preserved in cold 5% formalin
STOOL ANALYSIS
A stool analysis is a series of tests done on a stool (feces) sample to help diagnose certain conditions affecting the digestive tract .
These conditions can include infection (such as from parasites, viruses, or bacteria), poor nutrient absorption, or cancer.
Common Fecal Sample Examinations
Macroscopic Examination
Color
Consistency
Mucus and Blood
Other Abnormal features
adult worm or segment
Microscopic Examination
WBC/ HPF
RBC/ HPF
Yeast
Cyst, trophozoite, or both
Larvae, egg, or both
Chemical Examination
Fecal PH test
Fecal fatty acid testing
Testing feces for Occult Blood
Stool reducing substances testing
Bacteriological Culture When Indicate
Especially for Shigella and Salmonella Species
Macroscopic Examination
Color:
Brown is normal color, results from the intestinal oxidation of stercobilinogen to urobilin.
Bright red to dark red to black stools occur when iron or bismuth is taken or when there is intestinal hemorrhage.
Pale yellow stools indicate the biliary obstruction, steatorrea, and also associated with diagnostic procedures that use barium sulfate.
White stools occur when there is obstructive jaundice.
Green stool may observed in patient taking oral antibiotic, because of oxidation of bilirubin to biliverdin.
Consistency: degree of moisture, will be a guide as to whether the trophozoite stage or the cyst stage of protozoa is likely to present.
Formed, write “F”
Soft , write “S”
Loose , write “L”
Watery , write “W”
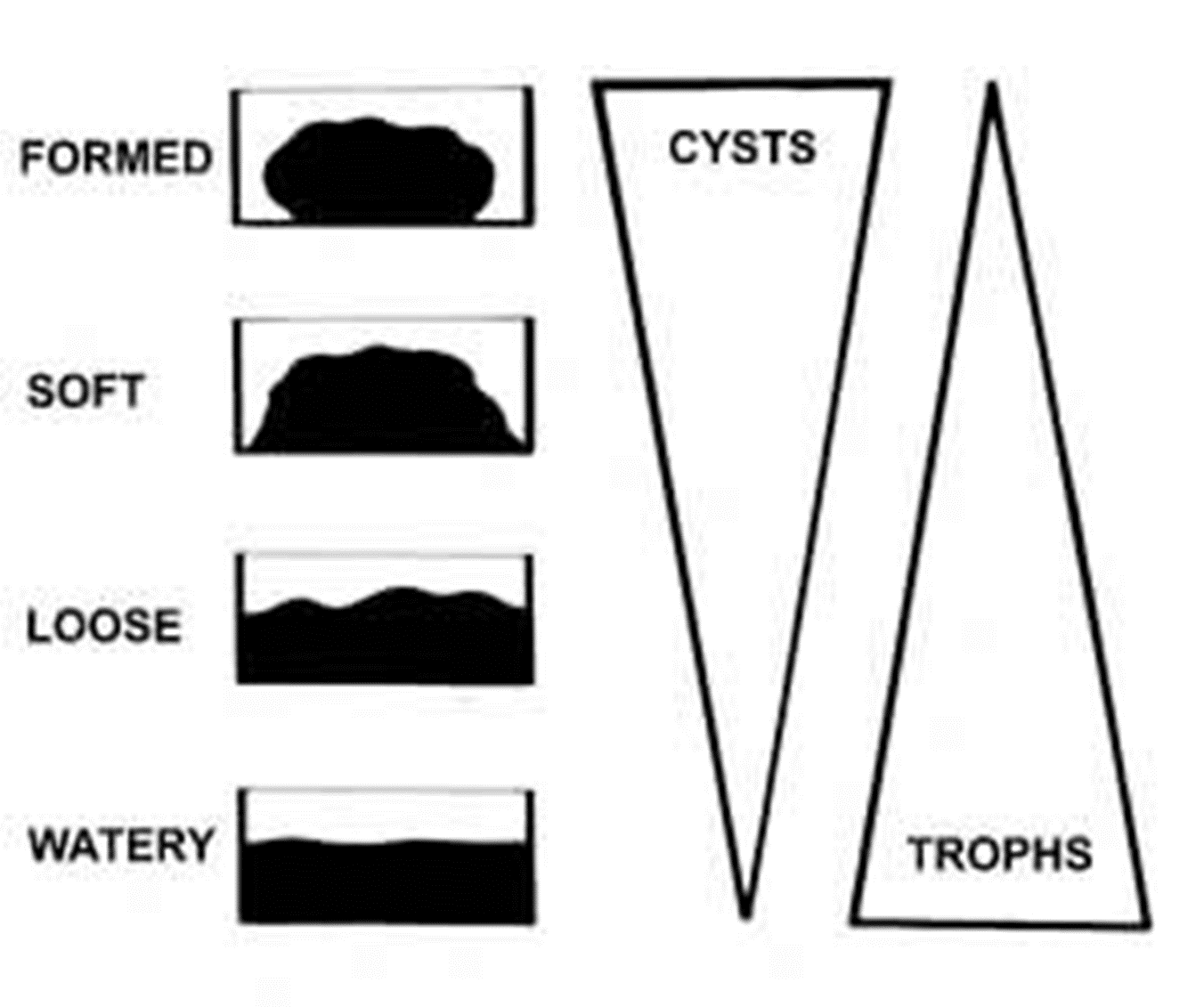
Image: Illustrating effects of the state of the consistence of the stool sample
Abnormal features:
If mucus is present writ “M”, and “B” if blood is present.
The presence of mucus coated stool is indicative for intestinal inflammation or irritation.
Adult worm or segments
The feces may have adult helminthes or segments present such as Ascaris lumbricoides, Entrobius vermicularis, or Taenia spp. gravid segment, these can be seen by naked eye.
And frequently motile for several days and may migrate to the top of the container.
Notice
If several specimens are received at the same time; those containing blood and mucus should be examined first, followed by liquid specimens. These specimens are the most likely to contain amoebic trophozoites ( which die soon after being passed), and must be examined within 1 hour after passage.
Formed specimens may be examined at any time during the first day, but should not be left overnight ( cyst may disintegrate).
Excessive bulky stools may indicate conditions such as giardiasis.
. Microscopic Examination of wet mount
Wet mount is the simplest and easiest technique for the examination of feces, and this method should be performed in all laboratories at peripheral level.
A wet mount can be prepared directly from fecal material or from concentrated specimens.
The basic types of wet mount that should be used for each fecal examination are normal saline (0.85% NaCl), iodine, and buffered methylene blue.
Home work. Read about

Laboratory analysis includes macroscopic, microscopic examination, chemical tests, and microbiologic tests.
The stool will be checked for color, consistency, weight (volume), shape, odor, and the presence of mucus and parasites stages.
The stool may be examined for hidden (occult) blood, fat, meat fibers, bile, white blood cells, and sugars called reducing substances.
The pH of the stool also may be measured.
A stool culture is done to find out if bacteria may be causing an infection.
The Saline Wet Mount
Is used for the initial microscopic examination of stool specimens.
It is employed primarily to demonstrate worms eggs, larvae. Protozoan trophozoites, and cysts.
This type of mount can also reveal the presence of red blood cells and white blood cells.
If the presence of amoebic trophozoites is suspected, warm saline (37˚C) should be used.
The Iodine Wet Mount
Is used mainly to stain glycogen and the nuclei of cysts, if present.
Cysts can usually be specifically identified in this mount.
Trophozoite can not be revealed by this type of wet mount, because iodine kill trophozoite.
The Buffered Methylene Blue Wet Mount
Should be prepared each time amoebic trophozoites are seen in a saline wet mount, or when their presence is suspected.
BMB stains amoebic trophozoites, but not stain amoebic cysts, flagellate trophozoites or flagellate cysts.
BMB stain is appropriate only for fresh unpreserved specimens.
BMB stain live organism only, it isn’t used on preserved samples in which the organism have been killed
Wait for five minutes to allow the stain to penetrate the trophozoites. It will overstrain the trophozoites in 30 minutes.
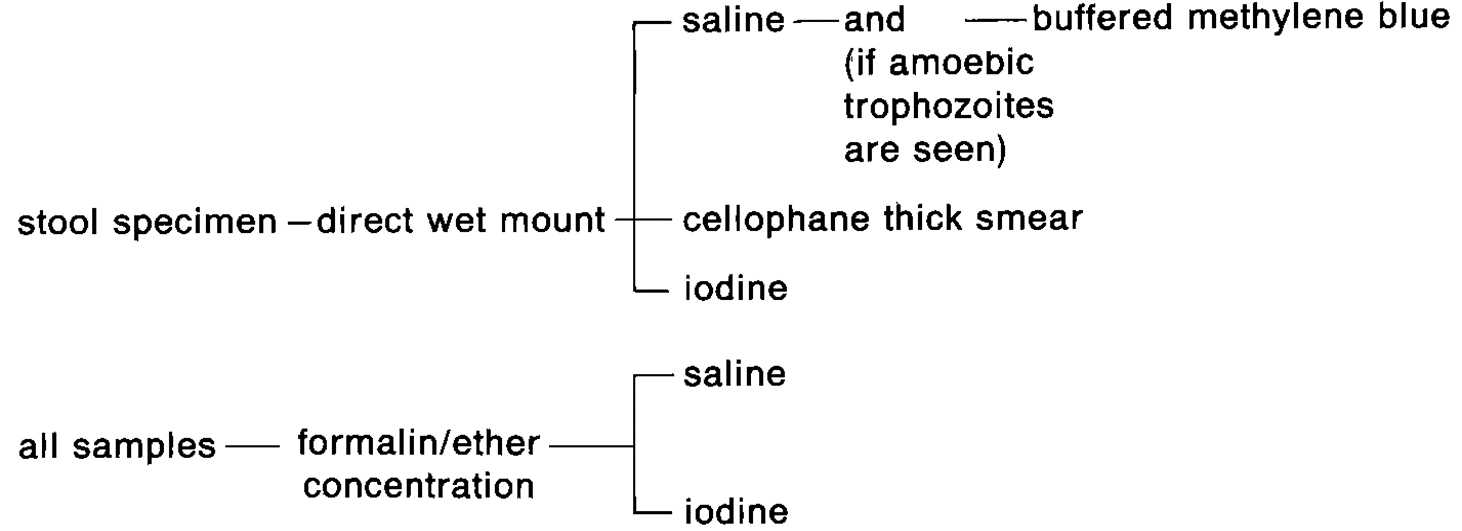
Image: Amounts from Direct Fresh Unpreserved Samples and Preserved Samples
Remember to read the Kato technique
Laboratory sampling
Formed stool: take the portion of stool from an area to include inside and outside parts of the specimen.
Stool with mucus: if mucus is present, label a second slide with the patient’s name or number. Put a drop of saline on the slide, pick up a small portion of mucus and mix with the saline. Trophozoites, if present, are sometimes more readily found in mucus than in the solid parts of the stool.
Loose watery stool: if mucus is not present, pick up a small portion of the stool (any part) and mix with the saline.
Making Direct smear Microscopy
Materials and reagents:
Microscopic slides.
Cover slips.
Applicator sticks.
Marker or pen for labeling.
Reagents:
Saline solution(isotonic)
Lugols iodine(1% solution)
BMB
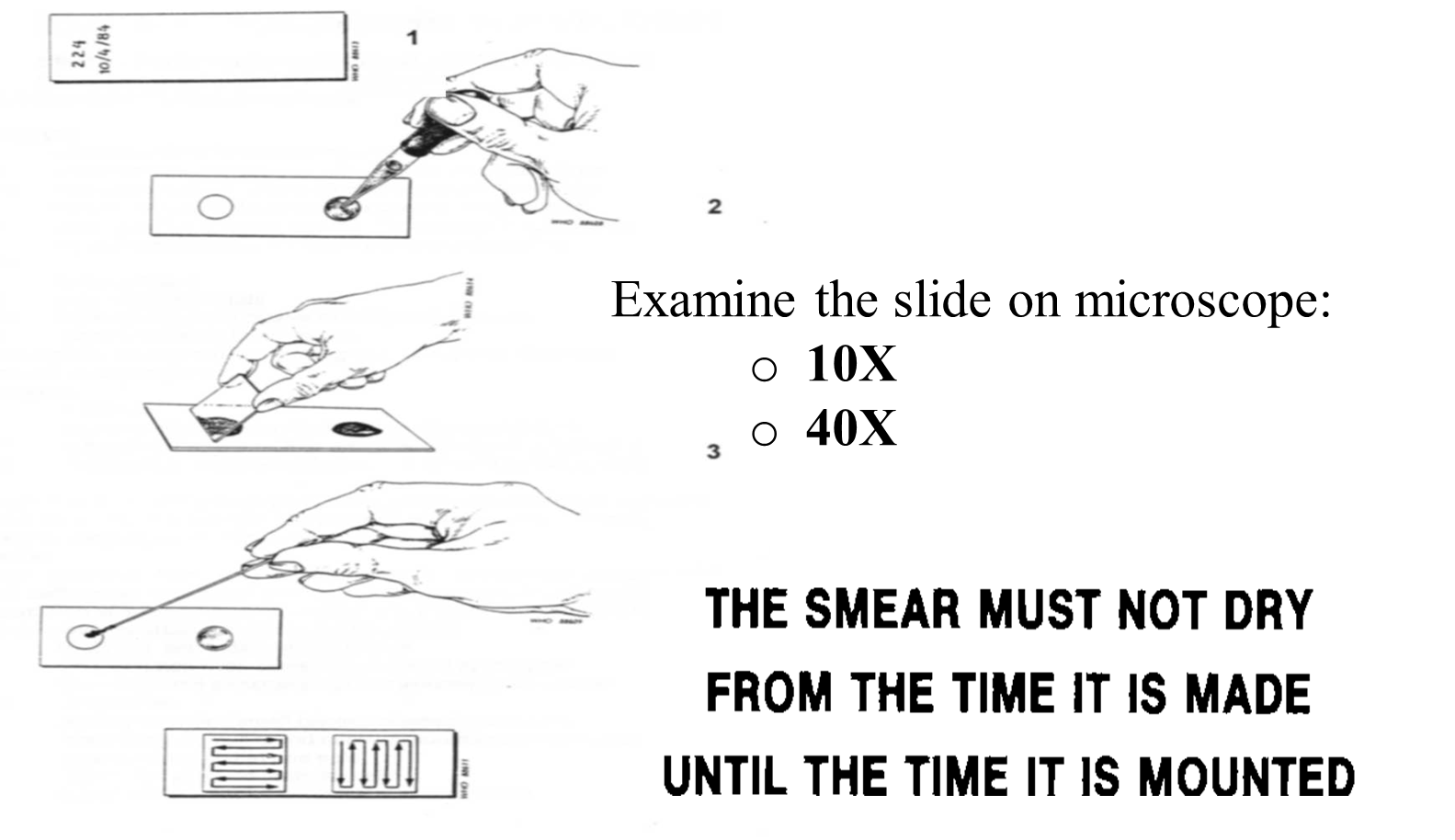
Image: summary of Wet Amounts Procedure
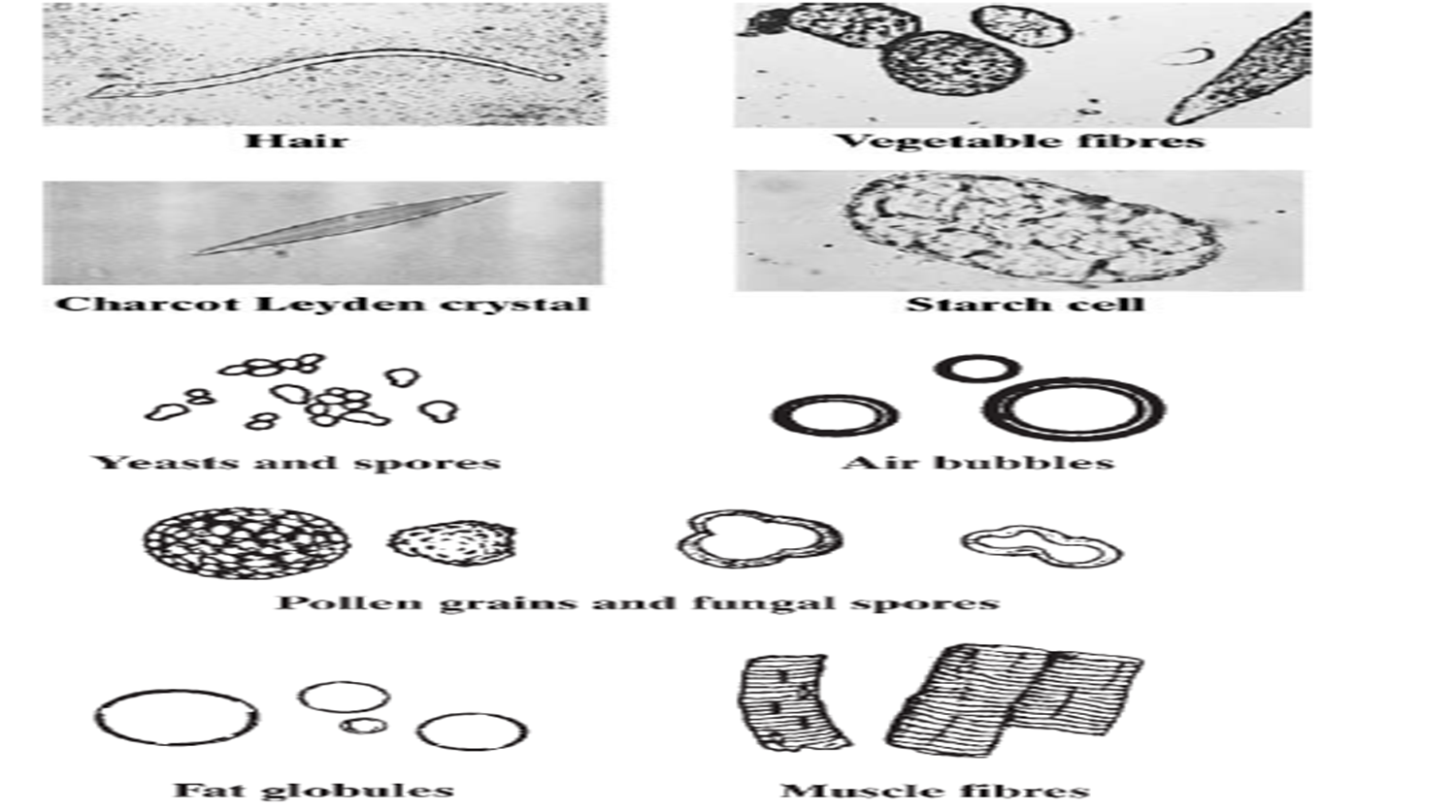
Image: Plate Structures found in faeces that required differentiation from parasites.

Result of Examination
If no parasites are found:
“No ova or parasites seen”, and specify whether this result was obtained by direct examination or by a concentration method (name method used).
Never state categorically: “No parasites”
If any parasites are seen, write the scientific name of the parasite with stages, Example: Giardia lambilia cyst with estimations as shown below:
Scanty . . . . . . . . . . . . . . . . 1–3 per preparation
Few . . . . . . . . . . . . . . . . . 4–10 per preparation
Moderate number . . . . 11–20 per preparation
Many . . . . . . . . . . . . . . . 21–40 per preparation
Very many . . . . . . . . . over 40 per preparation
SELF DIRECTED STUDY
Counting of Helminthes Eggs in Feces
Permanent stains, preparation of smears and staining
Collection, preparation (both wet amounts and permanent smears) of other samples and examination
These will be included in your CATs and Final Examinations
Last modified: Wednesday, 24 June 2026, 8:52 PM
Background Colour
Font Face
Font Kerning
Font Size
1
Image Visibility
Letter Spacing
0
Line Height
1.2
Link Highlight
Text Alignment
Text Colour